

Verbal autopsy as a tool for identifying children dying of sickle cell disease: a validation study conducted in Kilifi district, Kenya
- PMID: 24755265
- PMCID: PMC4022330
- DOI: 10.1186/1741-7015-12-65
Verbal autopsy as a tool for identifying children dying of sickle cell disease: a validation study conducted in Kilifi district, Kenya
Abstract
Background: Sickle cell disease (SCD) is common in many parts of sub-Saharan Africa (SSA), where it is associated with high early mortality. In the absence of newborn screening, most deaths among children with SCD go unrecognized and unrecorded. As a result, SCD does not receive the attention it deserves as a leading cause of death among children in SSA. In the current study, we explored the potential utility of verbal autopsy (VA) as a tool for attributing underlying cause of death (COD) in children to SCD.
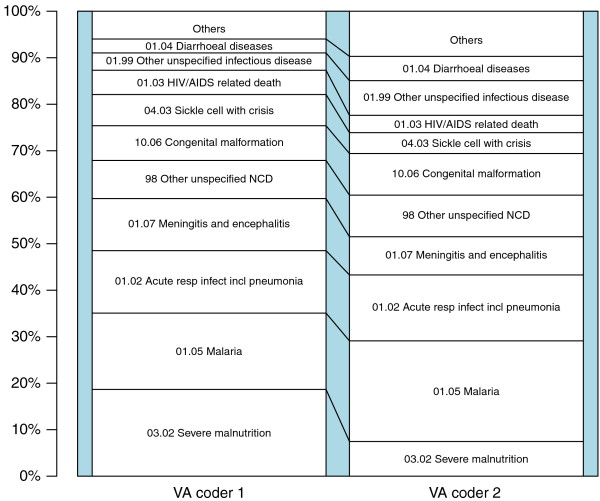
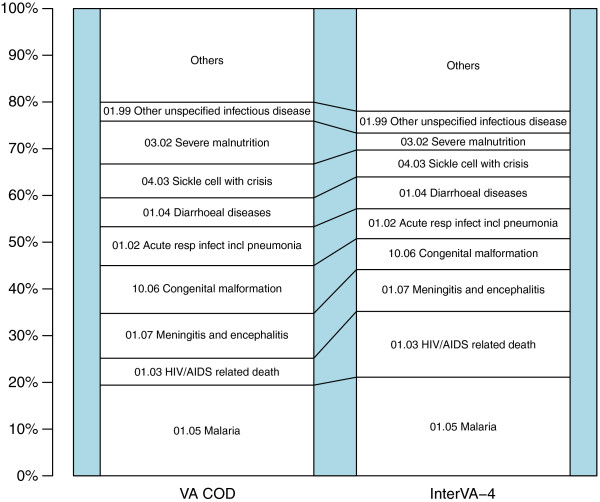
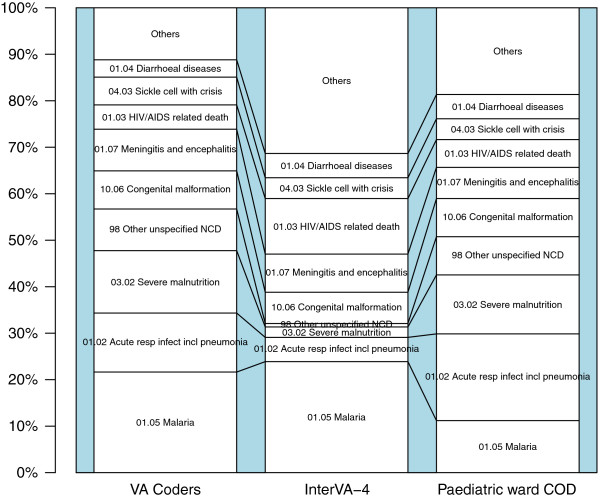
Methods: We used the 2007 WHO Sample Vital Registration with Verbal Autopsy (SAVVY) VA tool to determine COD among child residents of the Kilifi Health and Demographic Surveillance System (KHDSS), Kenya, who died between January 2008 and April 2011. VAs were coded both by physician review (physician coded verbal autopsy, PCVA) using COD categories based on the WHO International Classification of Diseases 10th Edition (ICD-10) and by using the InterVA-4 probabilistic model after extracting data according to the 2012 WHO VA standard. Both of these methods were validated against one of two gold standards: hospital ICD-10 physician-assigned COD for children who died in Kilifi District Hospital (KDH) and, where available, laboratory confirmed SCD status for those who died in the community.
Results: Overall, 6% and 5% of deaths were attributed to SCD on the basis of PCVA and the InterVA-4 model, respectively. Of the total deaths, 22% occurred in hospital, where the agreement coefficient (AC1) for SCD between PCVA and hospital physician diagnosis was 95.5%, and agreement between InterVA-4 and hospital physician diagnosis was 96.9%. Confirmatory laboratory evidence of SCD status was available for 15% of deaths, in which the AC1 against PCVA was 87.5%.
Conclusions: Other recent studies and provisional data from this study, outlining the importance of SCD as a cause of death in children in many parts of the developing world, contributed to the inclusion of specific SCD questions in the 2012 version of the WHO VA instruments, and a specific code for SCD has now been included in the WHO and InterVA-4 COD listings. With these modifications, VA may provide a useful approach to quantifying the contribution of SCD to childhood mortality in rural African communities. Further studies will be needed to evaluate the generalizability of our findings beyond our local context.
Figures
Similar articles
-
Validation of verbal autopsy methods for assessment of child mortality in sub-Saharan Africa and the policy implication: a rapid review.Pan Afr Med J. 2019 Aug 22;33:318. doi: 10.11604/pamj.2019.33.318.16405. eCollection 2019. Pan Afr Med J. 2019. PMID: 31692720 Free PMC article. Review.
-
Causes of death among persons of all ages within the Kilifi Health and Demographic Surveillance System, Kenya, determined from verbal autopsies interpreted using the InterVA-4 model.Glob Health Action. 2014 Oct 29;7:25593. doi: 10.3402/gha.v7.25593. eCollection 2014. Glob Health Action. 2014. PMID: 25377342 Free PMC article.
-
Validating physician-certified verbal autopsy and probabilistic modeling (InterVA) approaches to verbal autopsy interpretation using hospital causes of adult deaths.Popul Health Metr. 2011 Aug 5;9:49. doi: 10.1186/1478-7954-9-49. Popul Health Metr. 2011. PMID: 21819603 Free PMC article.
-
Agreement between cause of death assignment by computer-coded verbal autopsy methods and physician coding of verbal autopsy interviews in South Africa.Glob Health Action. 2023 Dec 31;16(1):2285105. doi: 10.1080/16549716.2023.2285105. Epub 2023 Dec 1. Glob Health Action. 2023. PMID: 38038664 Free PMC article.
-
Hydroxyurea for children with sickle cell disease in sub-Saharan Africa: A summary of the evidence, opportunities, and challenges.Pharmacotherapy. 2023 May;43(5):430-441. doi: 10.1002/phar.2792. Epub 2023 Mar 26. Pharmacotherapy. 2023. PMID: 36906823 Review.
Cited by
-
Validation of verbal autopsy methods for assessment of child mortality in sub-Saharan Africa and the policy implication: a rapid review.Pan Afr Med J. 2019 Aug 22;33:318. doi: 10.11604/pamj.2019.33.318.16405. eCollection 2019. Pan Afr Med J. 2019. PMID: 31692720 Free PMC article. Review.
-
Hydroxyurea for Children with Sickle Cell Anemia in Sub-Saharan Africa.N Engl J Med. 2019 Jan 10;380(2):121-131. doi: 10.1056/NEJMoa1813598. Epub 2018 Dec 1. N Engl J Med. 2019. PMID: 30501550 Free PMC article. Clinical Trial.
-
Causes of death among persons of all ages within the Kilifi Health and Demographic Surveillance System, Kenya, determined from verbal autopsies interpreted using the InterVA-4 model.Glob Health Action. 2014 Oct 29;7:25593. doi: 10.3402/gha.v7.25593. eCollection 2014. Glob Health Action. 2014. PMID: 25377342 Free PMC article.
-
Fifteen years of epidemiology in BMC Medicine.BMC Med. 2019 Sep 23;17(1):177. doi: 10.1186/s12916-019-1407-5. BMC Med. 2019. PMID: 31543077 Free PMC article.
-
Sickle cell disease: a neglected chronic disease of increasing global health importance.Arch Dis Child. 2015 Jan;100(1):48-53. doi: 10.1136/archdischild-2013-303773. Epub 2014 Sep 19. Arch Dis Child. 2015. PMID: 25239949 Free PMC article. Review.
References
-
- Piel FB, Patil AP, Howes RE, Nyangiri OA, Gething PW, Dewi M, Temperley WH, Williams TN, Weatherall DJ, Hay SI. Global epidemiology of sickle haemoglobin in neonates: a contemporary geostatistical model-based map and population estimates. Lancet. 2013;381:142–151. doi: 10.1016/S0140-6736(12)61229-X. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
