

Identifying unusual performance in Australian and New Zealand intensive care units from 2000 to 2010
- PMID: 24755369
- PMCID: PMC4021168
- DOI: 10.1186/1471-2288-14-53
Identifying unusual performance in Australian and New Zealand intensive care units from 2000 to 2010
Abstract
Background: The Australian and New Zealand Intensive Care Society (ANZICS) Adult Patient Database (APD) collects voluntary data on patient admissions to Australian and New Zealand intensive care units (ICUs). This paper presents an in-depth statistical analysis of risk-adjusted mortality of ICU admissions from 2000 to 2010 for the purpose of identifying ICUs with unusual performance.
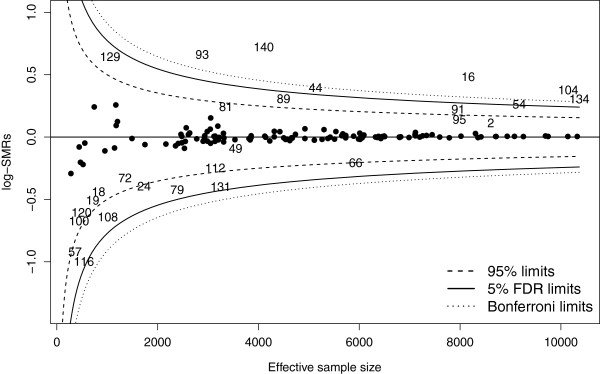
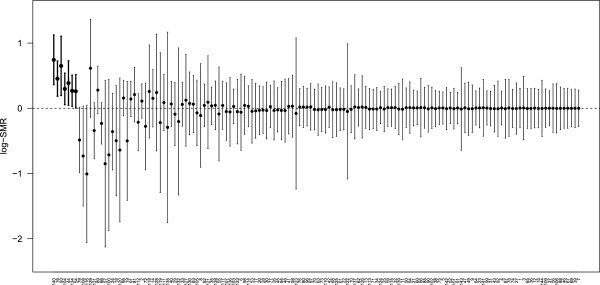
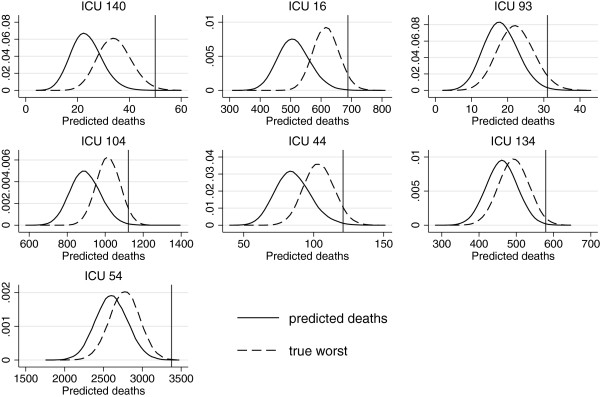
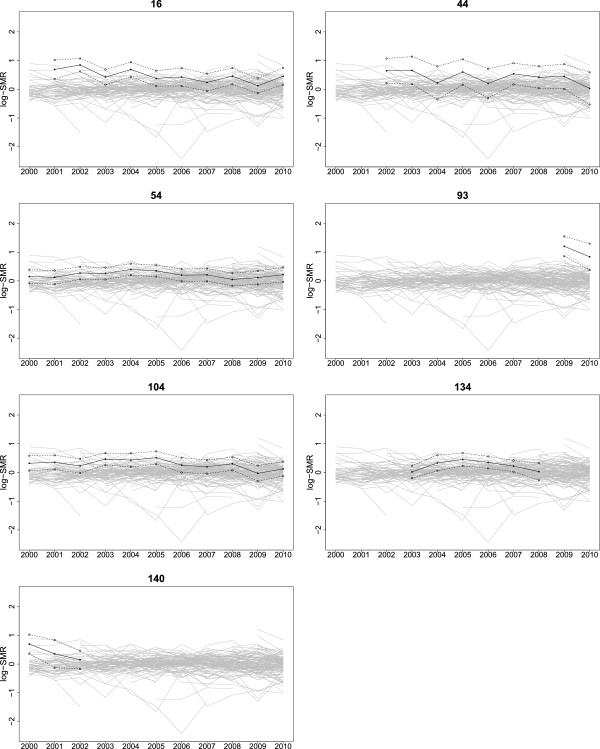
Methods: A cohort of 523,462 patients from 144 ICUs was analysed. For each ICU, the natural logarithm of the standardised mortality ratio (log-SMR) was estimated from a risk-adjusted, three-level hierarchical model. This is the first time a three-level model has been fitted to such a large ICU database anywhere. The analysis was conducted in three stages which included the estimation of a null distribution to describe usual ICU performance. Log-SMRs with appropriate estimates of standard errors are presented in a funnel plot using 5% false discovery rate thresholds. False coverage-statement rate confidence intervals are also presented. The observed numbers of deaths for ICUs identified as unusual are compared to the predicted true worst numbers of deaths under the model for usual ICU performance.
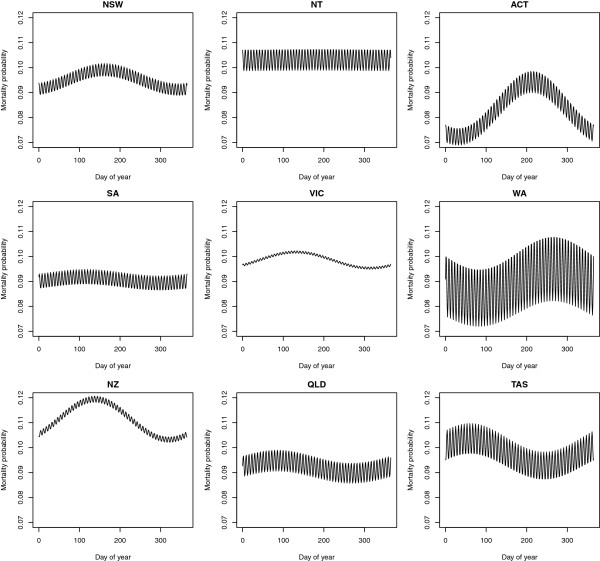
Results: Seven ICUs were identified as performing unusually over the period 2000 to 2010, in particular, demonstrating high risk-adjusted mortality compared to the majority of ICUs. Four of the seven were ICUs in private hospitals. Our three-stage approach to the analysis detected outlying ICUs which were not identified in a conventional (single) risk-adjusted model for mortality using SMRs to compare ICUs. We also observed a significant linear decline in mortality over the decade. Distinct yearly and weekly respiratory seasonal effects were observed across regions of Australia and New Zealand for the first time.
Conclusions: The statistical approach proposed in this paper is intended to be used for the review of observed ICU and hospital mortality. Two important messages from our study are firstly, that comprehensive risk-adjustment is essential in modelling patient mortality for comparing performance, and secondly, that the appropriate statistical analysis is complicated.
Figures
Similar articles
-
Fixed effects modelling for provider mortality outcomes: Analysis of the Australia and New Zealand Intensive Care Society (ANZICS) Adult Patient Data-base.PLoS One. 2014 Jul 16;9(7):e102297. doi: 10.1371/journal.pone.0102297. eCollection 2014. PLoS One. 2014. PMID: 25029164 Free PMC article.
-
Evaluating the performance of Australian and New Zealand intensive care units in 2009 and 2010.Stat Med. 2013 Sep 20;32(21):3720-36. doi: 10.1002/sim.5779. Epub 2013 Mar 25. Stat Med. 2013. PMID: 23526209
-
Mortality and length-of-stay outcomes, 1993-2003, in the binational Australian and New Zealand intensive care adult patient database.Crit Care Med. 2008 Jan;36(1):46-61. doi: 10.1097/01.CCM.0000295313.08084.58. Crit Care Med. 2008. PMID: 18090383
-
Identification and assessment of potentially high-mortality intensive care units using the ANZICS Centre for Outcome and Resource Evaluation clinical registry.Crit Care Resusc. 2017 Sep;19(3):230-238. Crit Care Resusc. 2017. PMID: 28866973
-
Noise in ICUs: Review and Detailed Analysis of Long-Term SPL Monitoring in ICUs in Northern Spain.Sensors (Basel). 2022 Nov 22;22(23):9038. doi: 10.3390/s22239038. Sensors (Basel). 2022. PMID: 36501740 Free PMC article. Review.
Cited by
-
Modelling hospital outcome: problems with endogeneity.BMC Med Res Methodol. 2021 Jun 21;21(1):124. doi: 10.1186/s12874-021-01251-8. BMC Med Res Methodol. 2021. PMID: 34154530 Free PMC article.
-
Fixed effects modelling for provider mortality outcomes: Analysis of the Australia and New Zealand Intensive Care Society (ANZICS) Adult Patient Data-base.PLoS One. 2014 Jul 16;9(7):e102297. doi: 10.1371/journal.pone.0102297. eCollection 2014. PLoS One. 2014. PMID: 25029164 Free PMC article.
-
Variation in severity-adjusted resource use and outcome in intensive care units.Intensive Care Med. 2022 Jan;48(1):67-77. doi: 10.1007/s00134-021-06546-4. Epub 2021 Oct 18. Intensive Care Med. 2022. PMID: 34661693 Free PMC article.
-
Evaluations of statistical methods for outlier detection when benchmarking in clinical registries: a systematic review.BMJ Open. 2023 Jul 14;13(7):e069130. doi: 10.1136/bmjopen-2022-069130. BMJ Open. 2023. PMID: 37451708 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
