

Fetal growth and risk of stillbirth: a population-based case-control study
- PMID: 24755550
- PMCID: PMC3995658
- DOI: 10.1371/journal.pmed.1001633
Fetal growth and risk of stillbirth: a population-based case-control study
Abstract
Background: Stillbirth is strongly related to impaired fetal growth. However, the relationship between fetal growth and stillbirth is difficult to determine because of uncertainty in the timing of death and confounding characteristics affecting normal fetal growth.
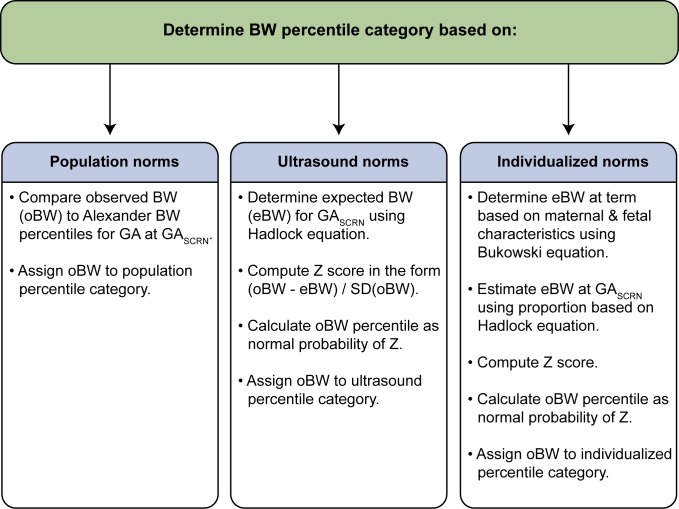
Methods and findings: We conducted a population-based case-control study of all stillbirths and a representative sample of live births in 59 hospitals in five geographic areas in the US. Fetal growth abnormalities were categorized as small for gestational age (SGA) (<10th percentile) or large for gestational age (LGA) (>90th percentile) at death (stillbirth) or delivery (live birth) using population, ultrasound, and individualized norms. Gestational age at death was determined using an algorithm that considered the time-of-death interval, postmortem examination, and reliability of the gestational age estimate. Data were weighted to account for the sampling design and differential participation rates in various subgroups. Among 527 singleton stillbirths and 1,821 singleton live births studied, stillbirth was associated with SGA based on population, ultrasound, and individualized norms (odds ratio [OR] [95% CI]: 3.0 [2.2 to 4.0]; 4.7 [3.7 to 5.9]; 4.6 [3.6 to 5.9], respectively). LGA was also associated with increased risk of stillbirth using ultrasound and individualized norms (OR [95% CI]: 3.5 [2.4 to 5.0]; 2.3 [1.7 to 3.1], respectively), but not population norms (OR [95% CI]: 0.6 [0.4 to 1.0]). The associations were stronger with more severe SGA and LGA (<5th and >95th percentile). Analyses adjusted for stillbirth risk factors, subset analyses excluding potential confounders, and analyses in preterm and term pregnancies showed similar patterns of association. In this study 70% of cases and 63% of controls agreed to participate. Analysis weights accounted for differences between consenting and non-consenting women. Some of the characteristics used for individualized fetal growth estimates were missing and were replaced with reference values. However, a sensitivity analysis using individualized norms based on the subset of stillbirths and live births with non-missing variables showed similar findings.
Conclusions: Stillbirth is associated with both growth restriction and excessive fetal growth. These findings suggest that, contrary to current practices and recommendations, stillbirth prevention strategies should focus on both severe SGA and severe LGA pregnancies. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- MacDorman MF, Kirmeyer S (2009) Fetal and perinatal mortality, United States, 2005. Natl Vital Stat Rep 57: 1–19. - PubMed
-
- MacDorman MF, Mathews TJ (2008) Recent trends in infant mortality in the United States. NCHS Data Brief 1–8. - PubMed
-
- Lawn JE, Blencowe H, Pattinson R, Cousens S, Kumar R, et al. (2011) Stillbirths: Where? When? Why? How to make the data count? Lancet 377: 1448–1463 doi:10.1016/S0140-6736(10)62187-3 - DOI - PubMed
-
- Stanton C, Lawn JE, Rahman H, Wilczynska-Ketende K, Hill K (2006) Stillbirth rates: delivering estimates in 190 countries. Lancet 367: 1487–1494 doi:10.1016/S0140-6736(06)68586-3 - DOI - PubMed
-
- Flenady V, Koopmans L, Middleton P, Froen JF, Smith GC, et al. (2011) Major risk factors for stillbirth in high-income countries: a systematic review and meta-analysis. Lancet 377: 1331–1340 doi:10.1016/S0140-6736(10)62233-7 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
