

Predicting risk of postoperative lung injury in high-risk surgical patients: a multicenter cohort study
- PMID: 24755786
- PMCID: PMC3999474
- DOI: 10.1097/ALN.0000000000000216
Predicting risk of postoperative lung injury in high-risk surgical patients: a multicenter cohort study
Abstract
Background: Acute respiratory distress syndrome (ARDS) remains a serious postoperative complication. Although ARDS prevention is a priority, the inability to identify patients at risk for ARDS remains a barrier to progress. The authors tested and refined the previously reported surgical lung injury prediction (SLIP) model in a multicenter cohort of at-risk surgical patients.
Methods: This is a secondary analysis of a multicenter, prospective cohort investigation evaluating high-risk patients undergoing surgery. Preoperative ARDS risk factors and risk modifiers were evaluated for inclusion in a parsimonious risk-prediction model. Multiple imputation and domain analysis were used to facilitate development of a refined model, designated SLIP-2. Area under the receiver operating characteristic curve and the Hosmer-Lemeshow goodness-of-fit test were used to assess model performance.
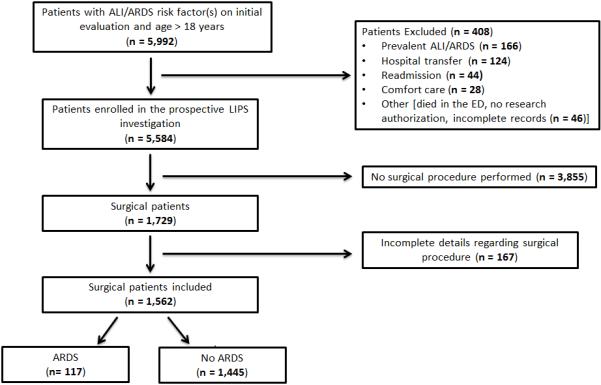
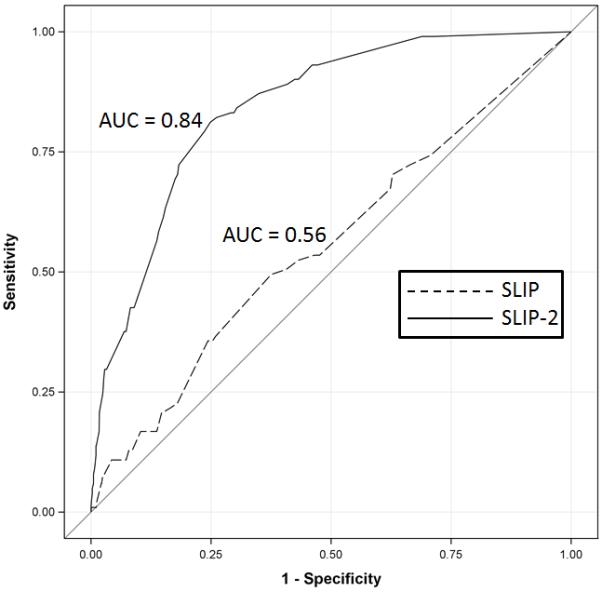
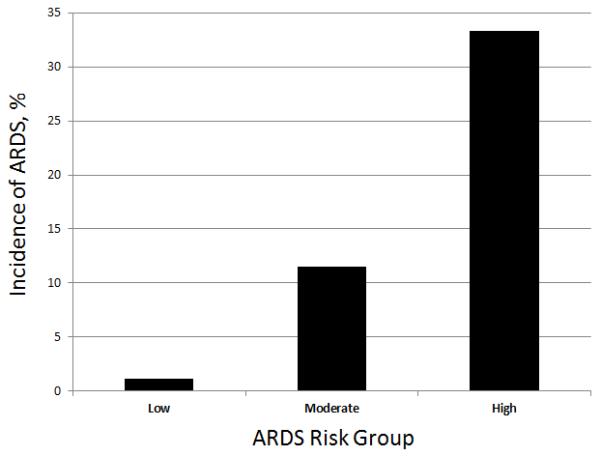
Results: Among 1,562 at-risk patients, ARDS developed in 117 (7.5%). Nine independent predictors of ARDS were identified: sepsis, high-risk aortic vascular surgery, high-risk cardiac surgery, emergency surgery, cirrhosis, admission location other than home, increased respiratory rate (20 to 29 and ≥30 breaths/min), FIO2 greater than 35%, and SpO2 less than 95%. The original SLIP score performed poorly in this heterogeneous cohort with baseline risk factors for ARDS (area under the receiver operating characteristic curve [95% CI], 0.56 [0.50 to 0.62]). In contrast, SLIP-2 score performed well (area under the receiver operating characteristic curve [95% CI], 0.84 [0.81 to 0.88]). Internal validation indicated similar discrimination, with an area under the receiver operating characteristic curve of 0.84.
Conclusions: In this multicenter cohort of patients at risk for ARDS, the SLIP-2 score outperformed the original SLIP score. If validated in an independent sample, this tool may help identify surgical patients at high risk for ARDS.
Figures
Comment in
-
Transforming high risk to high yield.Anesthesiology. 2014 May;120(5):1072-4. doi: 10.1097/ALN.0000000000000217. Anesthesiology. 2014. PMID: 24755782 Free PMC article. No abstract available.
Similar articles
-
Derivation and diagnostic accuracy of the surgical lung injury prediction model.Anesthesiology. 2011 Jul;115(1):117-28. doi: 10.1097/ALN.0b013e31821b5839. Anesthesiology. 2011. PMID: 21694510 Free PMC article.
-
Acute Respiratory Distress Syndrome Prediction Score: Derivation and Validation.Am J Crit Care. 2021 Jan 1;30(1):64-71. doi: 10.4037/ajcc2021753. Am J Crit Care. 2021. PMID: 33385206
-
SpO2/FiO2 ratio on hospital admission is an indicator of early acute respiratory distress syndrome development among patients at risk.J Intensive Care Med. 2015 May;30(4):209-16. doi: 10.1177/0885066613516411. Epub 2013 Dec 20. J Intensive Care Med. 2015. PMID: 24362445
-
Evaluation of prognostic risk models for postoperative pulmonary complications in adult patients undergoing major abdominal surgery: a systematic review and international external validation cohort study.Lancet Digit Health. 2022 Jul;4(7):e520-e531. doi: 10.1016/S2589-7500(22)00069-3. Lancet Digit Health. 2022. PMID: 35750401
-
Critical evaluation of established risk prediction models for acute respiratory distress syndrome in adult patients: A systematic review and meta-analysis.J Evid Based Med. 2023 Dec;16(4):465-476. doi: 10.1111/jebm.12565. Epub 2023 Dec 6. J Evid Based Med. 2023. PMID: 38058055
Cited by
-
Airway Pressure Release Ventilation Mode Improves Circulatory and Respiratory Function in Patients After Cardiopulmonary Bypass, a Randomized Trial.Front Physiol. 2021 Jun 3;12:684927. doi: 10.3389/fphys.2021.684927. eCollection 2021. Front Physiol. 2021. PMID: 34149459 Free PMC article.
-
Emerging therapies for the prevention of acute respiratory distress syndrome.Ther Adv Respir Dis. 2015 Aug;9(4):173-87. doi: 10.1177/1753465815585716. Epub 2015 May 22. Ther Adv Respir Dis. 2015. PMID: 26002528 Free PMC article. Review.
-
ARDS in Obese Patients: Specificities and Management.Crit Care. 2019 Mar 9;23(1):74. doi: 10.1186/s13054-019-2374-0. Crit Care. 2019. PMID: 30850002 Free PMC article. Review.
-
External validation of the CARDOT score for predicting respiratory complications after thoracic surgery.BMC Anesthesiol. 2024 Aug 30;24(1):301. doi: 10.1186/s12871-024-02685-5. BMC Anesthesiol. 2024. PMID: 39215223 Free PMC article.
-
Outcome of veno-venous extracorporeal membrane oxygenation use in acute respiratory distress syndrome after cardiac surgery with cardiopulmonary bypass.J Thorac Dis. 2016 Jul;8(7):1804-13. doi: 10.21037/jtd.2016.05.86. J Thorac Dis. 2016. PMID: 27499972 Free PMC article.
References
-
- Fernandez-Perez ER, Sprung J, Afessa B, Warner DO, Vachon CM, Schroeder DR, Brown DR, Hubmayr RD, Gajic O. Intraoperative ventilator settings and acute lung injury after elective surgery: A nested case control study. Thorax. 2009;64:121–7. - PubMed
-
- Alam N, Park BJ, Wilton A, Seshan VE, Bains MS, Downey RJ, Flores RM, Rizk N, Rusch VW, Amar D. Incidence and risk factors for lung injury after lung cancer resection. Ann Thorac Surg. 2007;84:1085–91. - PubMed
-
- Herridge MS, Tansey CM, Matte A, Tomlinson G, Diaz-Granados N, Cooper A, Guest CB, Mazer CD, Mehta S, Stewart TE, Kudlow P, Cook D, Slutsky AS, Cheung AM, Canadian Critical Care Trials Group Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364:1293–304. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
