

The idiopathic intracranial hypertension treatment trial: clinical profile at baseline
- PMID: 24756302
- PMCID: PMC4351808
- DOI: 10.1001/jamaneurol.2014.133
The idiopathic intracranial hypertension treatment trial: clinical profile at baseline
Abstract
Importance: To our knowledge, there are no large prospective cohorts of untreated patients with idiopathic intracranial hypertension (IIH) to characterize the disease.
Objective: To report the baseline clinical and laboratory features of patients enrolled in the Idiopathic Intracranial Hypertension Treatment Trial.
Design, setting, and participants: We collected data at baseline from questionnaires, examinations, automated perimetry, and fundus photography grading. Patients (n = 165) were enrolled from March 17, 2010, to November 27, 2012, at 38 academic and private practice sites in North America. All participants met the modified Dandy criteria for IIH and had a perimetric mean deviation between -2 dB and -7 dB. All but 4 participants were women.
Main outcomes and measures: Baseline and laboratory characteristics.
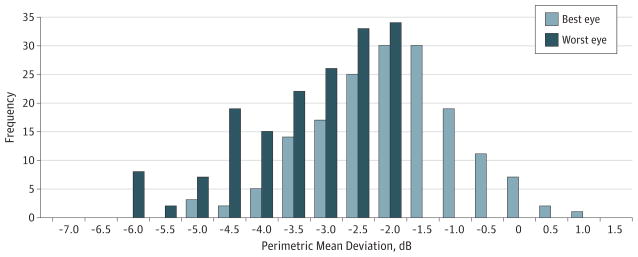
Results: The mean (SD) age of our patients was 29.0 (7.4) years and 4 (2.4%) were men. The average (SD) body mass index (calculated as weight in kilograms divided by height in meters squared) was 39.9 (8.3). Headache was the most common symptom (84%). Transient visual obscurations occurred in 68% of patients, back pain in 53%, and pulse synchronous tinnitus in 52%. Only 32% reported visual loss. The average (SD) perimetric mean deviation in the worst eye was -3.5 (1.1) dB, (range, -2.0 to -6.4 dB) and in the best eye was -2.3 (1.1) dB (range, -5.2 to 0.8 dB). A partial arcuate visual field defect with an enlarged blind spot was the most common perimetric finding. Visual acuity was 85 letters or better (20/20) in 71% of the worst eyes and 77% of the best eyes. Quality of life measures, including the National Eye Institute Visual Function Questionnaire-25 and the Short Form-36 physical and mental health summary scales, were lower compared with population norms.
Conclusions and relevance: The Idiopathic Intracranial Hypertension Treatment Trial represents the largest prospectively analyzed cohort of untreated patients with IIH. Our data show that IIH is almost exclusively a disease of obese young women. Patients with IIH with mild visual loss have typical symptoms, may have mild acuity loss, and have visual field defects, with predominantly arcuate loss and enlarged blind spots that require formal perimetry for detection.
Trial registration: clinicaltrials.gov Identifier: NCT01003639.
Conflict of interest statement
Figures




Comment in
-
Idiopathic intracranial hypertension: important questions answered with more to come.JAMA Neurol. 2014 Jun;71(6):678-80. doi: 10.1001/jamaneurol.2014.444. JAMA Neurol. 2014. PMID: 24756224 No abstract available.
-
Treating idiopathic intracranial hypertension.JAMA Neurol. 2014 Oct;71(10):1326-7. doi: 10.1001/jamaneurol.2014.2360. JAMA Neurol. 2014. PMID: 25322316 No abstract available.
-
Treating idiopathic intracranial hypertension--reply.JAMA Neurol. 2014 Oct;71(10):1327-8. doi: 10.1001/jamaneurol.2014.2363. JAMA Neurol. 2014. PMID: 25322318 No abstract available.
References
-
- Smith JL. Whence pseudotumor cerebri? J Clin Neuroophthalmol. 1985;5(1):55–56. - PubMed
-
- Durcan FJ, Corbett JJ, Wall M. The incidence of pseudotumor cerebri: population studies in Iowa and Louisiana. Arch Neurol. 1988;45(8):875–877. - PubMed
-
- Wall M, George D. Idiopathic intracranial hypertension: a prospective study of 50 patients. Brain. 1991;114(pt 1A):155–180. - PubMed
-
- Corbett JJ, Savino PJ, Thompson HS, et al. Visual loss in pseudotumor cerebri: follow-up of 57 patients from five to 41 years and a profile of 14 patients with permanent severe visual loss. Arch Neurol. 1982;39(8):461–474. - PubMed
-
- Lueck C, McIlwaine G. Interventions for idiopathic intracranial hypertension. Cochrane Database Syst Rev. 2005;(3):CD003434. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
