

Effect of acetazolamide on visual function in patients with idiopathic intracranial hypertension and mild visual loss: the idiopathic intracranial hypertension treatment trial
- PMID: 24756514
- PMCID: PMC4362615
- DOI: 10.1001/jama.2014.3312
Effect of acetazolamide on visual function in patients with idiopathic intracranial hypertension and mild visual loss: the idiopathic intracranial hypertension treatment trial
Abstract
Importance: Acetazolamide is commonly used to treat idiopathic intracranial hypertension (IIH), but there is insufficient information to establish an evidence base for its use.
Objective: To determine whether acetazolamide is beneficial in improving vision when added to a low-sodium weight reduction diet in patients with IIH and mild visual loss.
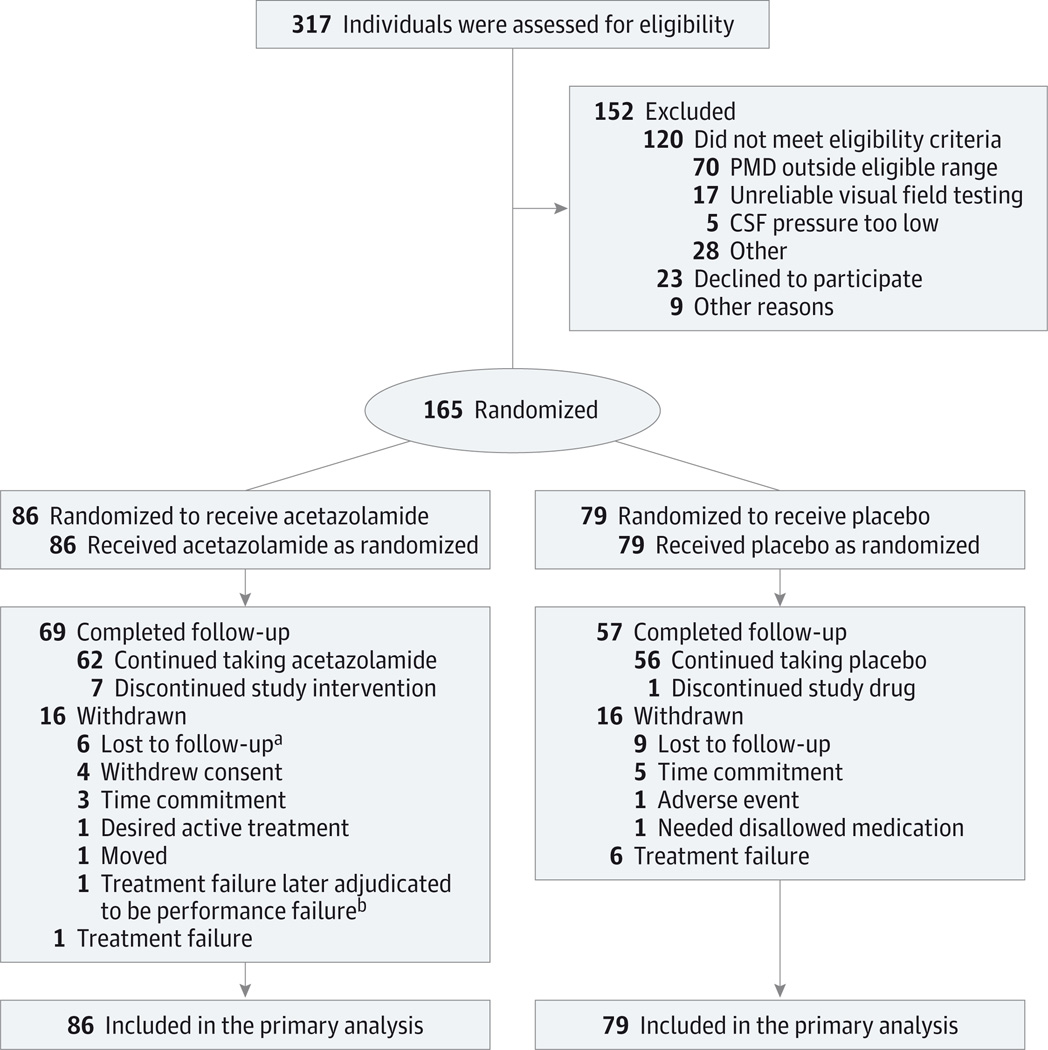
Design, setting, and participants: Multicenter, randomized, double-masked, placebo-controlled study of acetazolamide in 165 participants with IIH and mild visual loss who received a low-sodium weight-reduction diet. Participants were enrolled at 38 academic and private practice sites in North America from March 2010 to November 2012 and followed up for 6 months (last visit in June 2013). All participants met the modified Dandy criteria for IIH and had a perimetric mean deviation (PMD) between -2 dB and -7 dB. The mean age was 29 years and all but 4 participants were women.
Interventions: Low-sodium weight-reduction diet plus the maximally tolerated dosage of acetazolamide (up to 4 g/d) or matching placebo for 6 months.
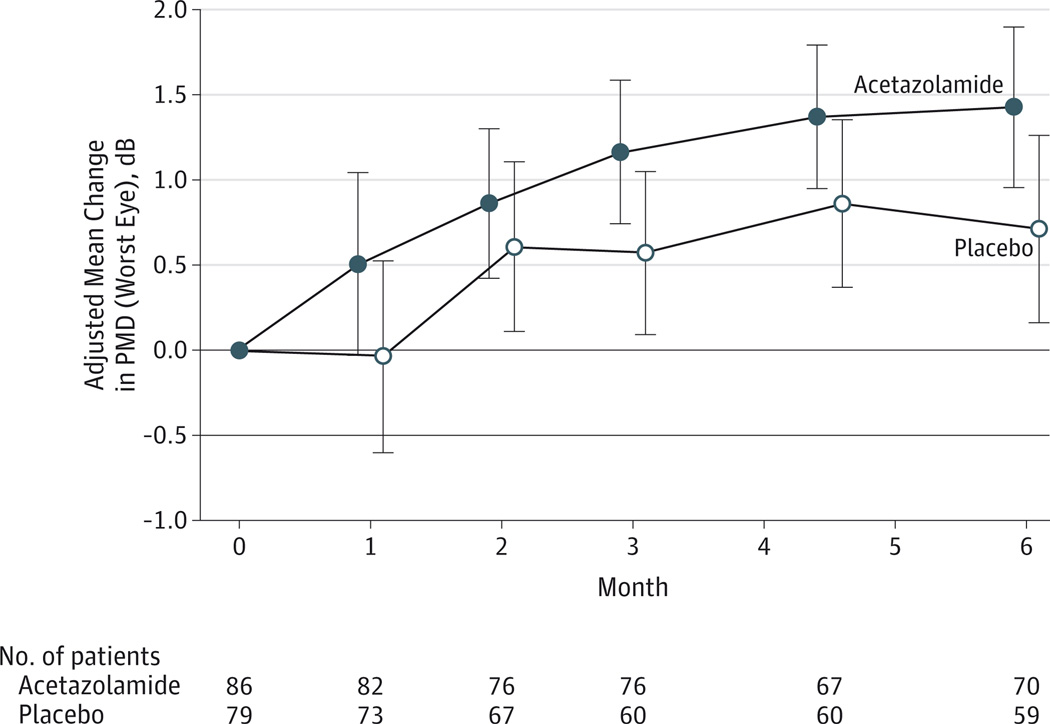
Main outcomes and measures: The planned primary outcome variable was the change in PMD from baseline to month 6 in the most affected eye, as measured by Humphrey Field Analyzer. Perimetric mean deviation is a measure of global visual field loss (mean deviation from age-corrected normal values), with a range of 2 to -32 dB; larger negative values indicate greater vision loss. Secondary outcome variables included changes in papilledema grade, quality of life (Visual Function Questionnaire 25 [VFQ-25] and 36-Item Short Form Health Survey), headache disability, and weight at month 6.
Results: The mean improvement in PMD was greater with acetazolamide (1.43 dB, from -3.53 dB at baseline to -2.10 dB at month 6; n = 86) than with placebo (0.71 dB, from -3.53 dB to -2.82 dB; n = 79); the difference was 0.71 dB (95% CI, 0 to 1.43 dB; P = .050). Mean improvements in papilledema grade (acetazolamide: -1.31, from 2.76 to 1.45; placebo: -0.61, from 2.76 to 2.15; treatment effect, -0.70; 95% CI, -0.99 to -0.41; P < .001) and vision-related quality of life as measured by the National Eye Institute VFQ-25 (acetazolamide: 8.33, from 82.97 to 91.30; placebo: 1.98, from 82.97 to 84.95; treatment effect, 6.35; 95% CI, 2.22 to 10.47; P = .003) and its 10-item neuro-ophthalmic supplement (acetazolamide: 9.82, from 75.45 to 85.27; placebo: 1.59, from 75.45 to 77.04; treatment effect, 8.23; 95% CI, 3.89 to 12.56; P < .001) were also observed with acetazolamide. Participants assigned to acetazolamide also experienced a reduction in weight (acetazolamide: -7.50 kg, from 107.72 kg to 100.22 kg; placebo: -3.45 kg, from 107.72 kg to 104.27 kg; treatment effect, -4.05 kg, 95% CI, -6.27 to -1.83 kg; P < .001).
Conclusions and relevance: In patients with IIH and mild visual loss, the use of acetazolamide with a low-sodium weight-reduction diet compared with diet alone resulted in modest improvement in visual field function. The clinical importance of this improvement remains to be determined.
Trial registration: clinicaltrials.gov Identifier: NCT01003639.
Conflict of interest statement
Figures
Comment in
-
Acetazolamide for pseudotumor cerebri: evidence from the NORDIC trial.JAMA. 2014 Apr 23-30;311(16):1618-9. doi: 10.1001/jama.2014.3325. JAMA. 2014. PMID: 24756510 Free PMC article. No abstract available.
-
Idiopathic intracranial hypertension.JAMA. 2014 Sep 10;312(10):1059-60. doi: 10.1001/jama.2014.8894. JAMA. 2014. PMID: 25203090 No abstract available.
-
Idiopathic intracranial hypertension--reply.JAMA. 2014 Sep 10;312(10):1060. doi: 10.1001/jama.2014.8903. JAMA. 2014. PMID: 25203092 No abstract available.
References
-
- Smith JL. Whence pseudotumor cerebri? J Clin Neuroophthalmol. 1985;5(1):55–56. - PubMed
-
- Newborg B. Pseudotumor cerebri treated by rice reduction diet. Arch Intern Med. 1974;133(5):802–807. - PubMed
-
- Johnson LN, Krohel GB, Madsen RW, March GA., Jr The role of weight loss and acetazolamide in the treatment of idiopathic intracranial hypertension (pseudotumor cerebri) Ophthalmology. 1998;105(12):2313–2317. - PubMed
-
- Vander Ark GD, Kempe LG, Smith DR. Pseudotumor cerebri treated with lumbar-peritoneal shunt. JAMA. 1971;217(13):1832–1834. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
