

Exchangeability in the case-crossover design
- PMID: 24756878
- PMCID: PMC4190513
- DOI: 10.1093/ije/dyu081
Exchangeability in the case-crossover design
Abstract
In cohort and case-control studies, confounding that arises as a result of differences in the distribution of determinants of the outcome between exposure groups leading to non-exchangeability are addressed by restriction, matching or with statistical models. In case-only studies, this issue is addressed by comparing each individual with his/herself. Although case-only designs use self-matching and only include individuals who develop the outcome of interest, issues of non-exchangeability are identical to those that arise in traditional case-control and cohort studies. In this review, we describe one type of case-only design, the case-crossover design, and discuss how the concept of exchangeability can be used to understand issues of confounding, carryover effects, period effects and selection bias in case-crossover studies.
Keywords: Epidemiology; case-crossover.
© The Author 2014; all rights reserved. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures
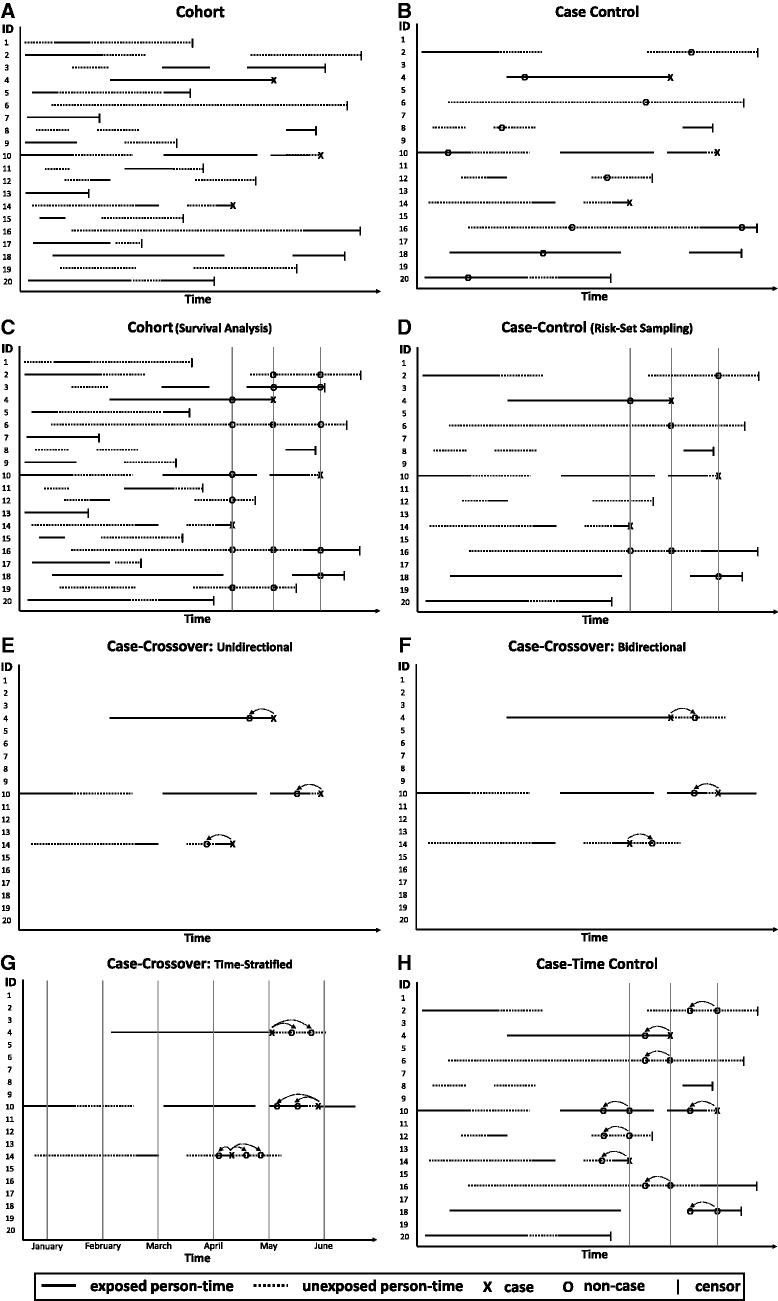
In a full cohort study (Panel A), the entire sample is followed for event occurrence; assumption of exchangeability between exposed and unexposed person-time in the entire study base.
In a case-control study with traditional incidence density sampling (Panel B), all or a random sample of the cases are identified and controls are sampled at random from the person-time at risk; assumption of exchangeability between exposed and unexposed person-time in the study base represented by the cases and sample of controls. Note that an individual can be randomly selected as a control and later become a case (ID#4) and an individual can be randomly selected as a control more than once (ID#16).
Non-exchangeability arising from changes over time can be addressed by matching on time using survival analysis methods in a cohort study (Panel C) or risk-set sampling in a case-control study (Panel D); assumption of exchangeability between exposed and unexposed person-time at the time the case occurred.
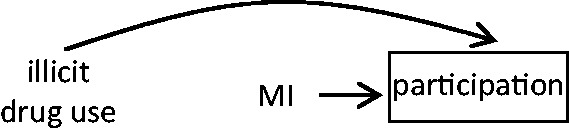
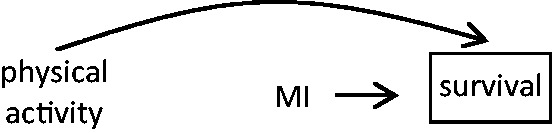
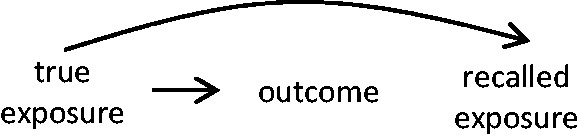
In a case-crossover study, non-exchangeability arising from slowly varying characteristics is eliminated by matching each case to himself/herself. If event occurrence affects subsequent exposure, a unidirectional case-crossover design (Panel E) is appropriate. Otherwise, a bidirectional case-crossover design (Panel F) can reduce exposure time trends by stratifying on the calendar month and then sampling person-time before and after the event (ID#4), before the event (ID#10) or after the event (ID#14)Assumption of exchangeability between exposed and unexposed person-time within each individual. Note that in the unidirectional design, individuals with no variation in exposure between the hazard and control periods do not contribute information to the estimator (ID#4).
In a case-crossover study, non-exchangeability arising from changes over time can be addressed by matching on time or by conducting a case-time control study (Panel G) that incorporates a control group. At the time the case occurs, obtain exposure information on cases and on controls for hazard periods and for control periods; exchangeability between exposed and unexposed person-time within each individual after accounting for a time-trend that is assumed to be the same for cases and controls.




References
-
- Becker NG, Salim A, Kelman CW. Analysis of a potential trigger of an acute illness. Biostatistics 2006;7:16–28 - PubMed
-
- Feldmann U. Design and analysis of drug safety studies, with special reference to sporadic drug use and acute adverse reactions. J Clin Epidemiol 1993;46:237–44 - PubMed
-
- Miettinen OS, Caro JJ. Principles of nonexperimental assessment of excess risk, with special reference to adverse drug reactions. J Clin Epidemiol 1989;42:325–31 - PubMed
-
- Maclure M. The case-crossover design: a method for studying transient effects on the risk of acute events. Am J Epidemiol 1991;133:144–53 - PubMed
-
- Suissa S. The case-time-control design. Epidemiology 1995;6: 248–53 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
