

Classification and characteristics of Japanese patients with antineutrophil cytoplasmic antibody-associated vasculitis in a nationwide, prospective, inception cohort study
- PMID: 24758294
- PMCID: PMC4060546
- DOI: 10.1186/ar4550
Classification and characteristics of Japanese patients with antineutrophil cytoplasmic antibody-associated vasculitis in a nationwide, prospective, inception cohort study
Abstract
Introduction: We investigated the clinical and serological features of patients with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) in Japan using data from a nationwide, prospective, inception cohort study.
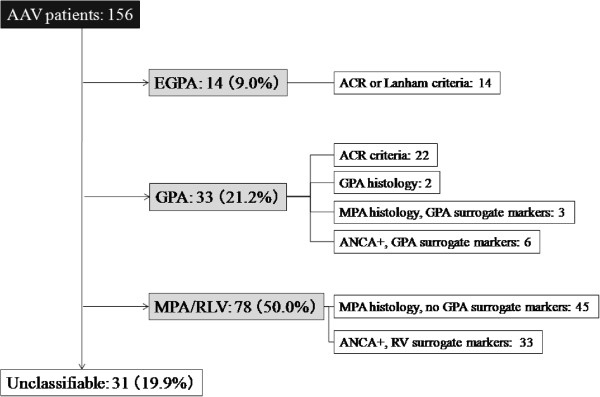
Methods: In total, 156 Japanese patients with newly diagnosed AAV were classified according to the European Medicines Agency (EMEA) algorithm with exploratory surrogate markers for AAV-related non-granulomatous pulmonary lesions, predefined as alveolar haemorrhage and interstitial lung disease (ILD), and their clinical and serological features were evaluated.
Results: Using the EMEA algorithm, we identified 14 patients (9.0%) with eosinophilic granulomatosis with polyangiitis (EGPA), 33 (21.2%) with granulomatosis with polyangiitis (GPA), 78 (50.0%) with microscopic polyangiitis and renal-limited vasculitis (MPA/RLV), and 31 (19.9%) with unclassifiable vasculitis. The average ages of patients with EGPA (male/female, 5/9), GPA (12/21), and MPA/RLV (35/43) and unclassifiable (9/22) were 58.0, 63.6, 71.1, and 70.6 years, respectively. Myeloperoxidase (MPO)-ANCA and proteinase-3 ANCA positivity was 50.0% and 0% for EGPA, 54.6% and 45.5% for GPA, 97.4% and 2.6% for MPA/RLV, and 93.5% and 3.2% for unclassifiable, respectively. According to the Birmingham Vasculitis Activity Score (BVAS), cutaneous (71.4%) and nervous system (92.9%) manifestations were prominent in EGPA and ear, nose, and throat manifestations (84.9%) and chest manifestations (66.7%) in GPA. Renal manifestations developed frequently in MPA/RLV (91.0%) and GPA (63.6%). The average serum creatinine levels were 0.71 mg/dL for EGPA, 1.51 mg/dL for GPA, 2.46 mg/dL for MPA/RLV, and 0.69 mg/dL for unclassifiable. The percentages of patients with ILD were 14.3% for EGPA, 9.0% for GPA, 47.4% for MPA/RLV, and 61.3% for unclassifiable. Patients with ILD (n = 61) had significantly lower BVAS (P = 0.019) with fewer ear, nose, and throat and cardiovascular manifestations than patients without ILD (n = 95).
Conclusions: MPO-ANCA-positive MPA/RLV is the most common form of AAV in Japanese patients, and one-half of patients with GPA were positive for MPO-ANCA. ILD is an important clinical manifestation in Japanese patients with AAV. Unclassifiable vasculitis with MPO-ANCA positivity and ILD may represent a novel variant of MPA.
Trial registration: The University Hospital Medical Information Network Clinical Trials Registry: UMIN000001648. Registered 28 February 2009.
Figures
References
-
- Jennette J, Falk R, Bacon P, Basu N, Cid M, Ferrario F, Flores-Suarez L, Gross W, Guillevin L, Hagen E, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA. Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65:1–11. - PubMed
-
- Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL, Hagen EC, Hoffman GS, Hunder GG, Kallenberg CG, McCluskey RT, Sinico RA, Rees AJ, van Es LA, Waldherr R, Wiik A. Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum. 1994;37:187–192. doi: 10.1002/art.1780370206. - DOI - PubMed
-
- Watts R, Lane S, Hanslik T, Hauser T, Hellmich B, Koldingsnes W, Mahr A, Segelmark M, Cohen-Tervaert JW, Scott D. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann Rheum Dis. 2007;66:222–227. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
