

Pulmonary arteriovenous malformations after the superior cavopulmonary shunt: mechanisms and clinical implications
- PMID: 24758411
- PMCID: PMC4410694
- DOI: 10.1586/14779072.2014.912132
Pulmonary arteriovenous malformations after the superior cavopulmonary shunt: mechanisms and clinical implications
Abstract
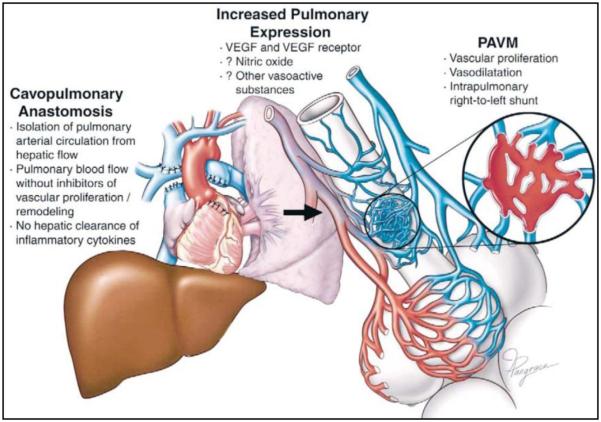
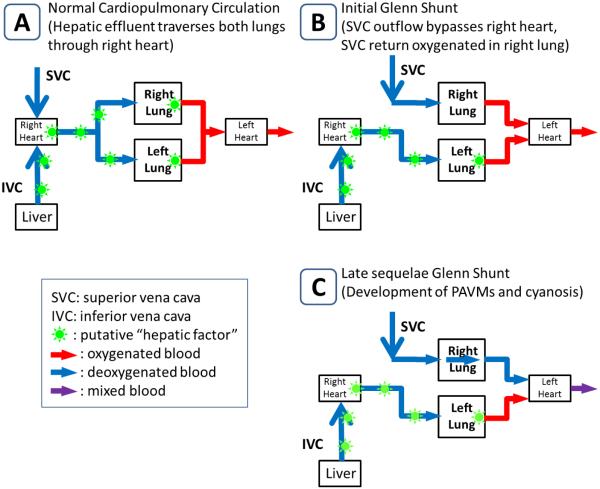
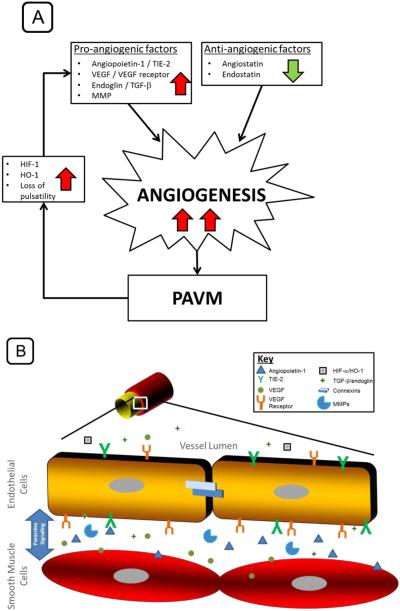
Children with functional single ventricle heart disease are commonly palliated down a staged clinical pathway toward a Fontan completion procedure (total cavopulmonary connection). The Fontan physiology is fraught with long-term complications associated with lower body systemic venous hypertension, eventually resulting in significant morbidity and mortality. The bidirectional Glenn shunt or superior cavopulmonary connection (SCPC) is commonly the transitional stage in single ventricle surgical management and provides excellent palliation. Some studies have demonstrated lower morbidity and mortality with the SCPC when compared with the Fontan. Unfortunately the durability of the SCPC is significantly limited by the development of pulmonary arteriovenous malformations (PAVMs) which have been commonly attributed to the absence of hepatic venous blood flow and the lack of pulsatile flow to the affected lungs. Abnormal angiogenesis has been suggested as a final common pathway to PAVM development. Understanding these fundamental mechanisms through the investigation of angiogenic pathways associated with the pathogenesis of PAVMs would help to develop medical therapies that could prevent or reverse this complication following SCPC. Such therapies could improve the longevity of the SCPC, potentially eliminate or significantly postpone the Fontan completion with its associated complications, and improve long-term survival in children with single ventricle disease.
Keywords: Fontan operation; angiogenesis; cavopulmonary connection; congenital heart disease; pulmonary arteriovenous malformations; single ventricle; superior.
Figures
Similar articles
-
Endostatin, an inhibitor of angiogenesis, decreases after bidirectional superior cavopulmonary anastamosis.Pediatr Cardiol. 2013 Feb;34(2):291-5. doi: 10.1007/s00246-012-0441-2. Epub 2012 Sep 8. Pediatr Cardiol. 2013. PMID: 22961274 Free PMC article.
-
Bidirectional cavopulmonary shunt in patients with anomalies of systemic and pulmonary venous drainage.Ann Thorac Surg. 1997 Jun;63(6):1676-84. doi: 10.1016/s0003-4975(97)00364-0. Ann Thorac Surg. 1997. PMID: 9205167 Clinical Trial.
-
Quantitative plasma proteomic analysis in children after superior cavopulmonary anastomosis with pulmonary arteriovenous malformations.Pediatr Res. 2025 Feb;97(3):1193-1198. doi: 10.1038/s41390-024-03450-7. Epub 2024 Aug 12. Pediatr Res. 2025. PMID: 39134758
-
Superior Cavopulmonary Connection: Its Physiology, Limitations, and Anesthetic Implications.Semin Cardiothorac Vasc Anesth. 2020 Dec;24(4):337-348. doi: 10.1177/1089253220939361. Epub 2020 Jul 9. Semin Cardiothorac Vasc Anesth. 2020. PMID: 32646291 Review.
-
Pulmonary arteriovenous malformations after cavopulmonary anastomosis.Ann Thorac Surg. 2003 Nov;76(5):1759-66. doi: 10.1016/s0003-4975(03)00450-8. Ann Thorac Surg. 2003. PMID: 14602341 Review.
Cited by
-
The Glenn procedure: Clinical outcomes in patients with congenital heart disease in pakistan.Ann Card Anaesth. 2021 Jan-Mar;24(1):30-35. doi: 10.4103/aca.ACA_85_19. Ann Card Anaesth. 2021. PMID: 33938828 Free PMC article.
-
Commentary: sVEGFR1 Is Enriched in Hepatic Vein Blood-Evidence for a Provisional Hepatic Factor Candidate?Front Pediatr. 2021 Nov 8;9:782779. doi: 10.3389/fped.2021.782779. eCollection 2021. Front Pediatr. 2021. PMID: 34820346 Free PMC article. No abstract available.
-
The Influence of Respiration on Blood Flow in the Fontan Circulation: Insights for Imaging-Based Clinical Evaluation of the Total Cavopulmonary Connection.Front Cardiovasc Med. 2021 Aug 5;8:683849. doi: 10.3389/fcvm.2021.683849. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34422920 Free PMC article. Review.
-
Collaterals in congenital heart disease: when and how to treat?Cardiovasc Diagn Ther. 2023 Apr 28;13(2):418-426. doi: 10.21037/cdt-23-10. Epub 2023 Mar 9. Cardiovasc Diagn Ther. 2023. PMID: 37583691 Free PMC article. Review.
-
Asking Bubbles for Direction: Assessment of a Classic Glenn Shunt Using Agitated Saline Contrast Echocardiography.CASE (Phila). 2020 Oct 1;4(6):485-489. doi: 10.1016/j.case.2020.09.002. eCollection 2020 Dec. CASE (Phila). 2020. PMID: 33376839 Free PMC article.
References
-
- Glenn WW. Circulatory bypass of the right side of the heart. IV. Shunt between superior vena cava and distal right pulmonary artery; report of clinical application. N Engl J Med. 1958;259(3):117–120. - PubMed
-
- Castaneda AR. From Glenn to Fontan. A continuing evolution. Circulation. 1992;86(5 Suppl):II80–84. - PubMed
-
- Jonas RA. Indications and timing for the bidirectional Glenn shunt versus the fenestrated Fontan circulation. J Thorac Cardiovasc Surg. 1994;108(3):522–524. - PubMed
-
- Hirsch JC, Goldberg C, Bove EL, et al. Fontan operation in the current era: a 15-year single institution experience. Ann Surg. 2008;248(3):402–410. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical