

Lung ultrasound for the diagnosis of pneumonia in adults: a systematic review and meta-analysis
- PMID: 24758612
- PMCID: PMC4005846
- DOI: 10.1186/1465-9921-15-50
Lung ultrasound for the diagnosis of pneumonia in adults: a systematic review and meta-analysis
Abstract
Background: Guidelines do not currently recommend the use of lung ultrasound (LUS) as an alternative to chest X-ray (CXR) or chest computerized tomography (CT) scan for the diagnosis of pneumonia. We conducted a meta-analysis to summarize existing evidence of the diagnostic accuracy of LUS for pneumonia in adults.
Methods: We conducted a systematic search of published studies comparing the diagnostic accuracy of LUS against a referent CXR or chest CT scan and/or clinical criteria for pneumonia in adults aged ≥18 years. Eligible studies were required to have a CXR and/or chest CT scan at the time of evaluation. We manually extracted descriptive and quantitative information from eligible studies, and calculated pooled sensitivity and specificity using the Mantel-Haenszel method and pooled positive and negative likelihood ratios (LR) using the DerSimonian-Laird method. We assessed for heterogeneity using the Q and I2 statistics.
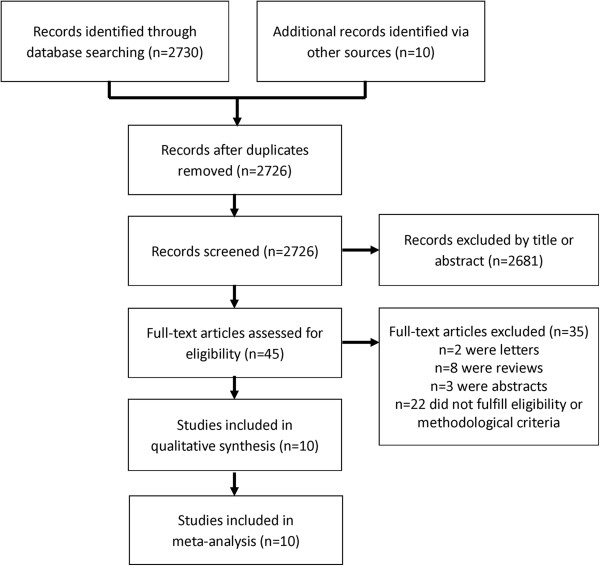
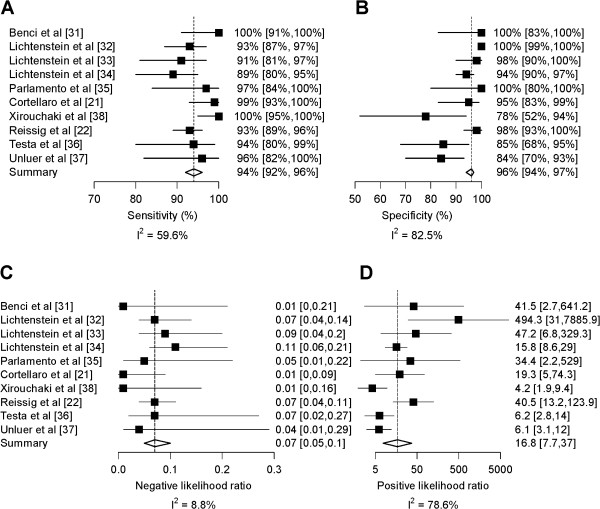
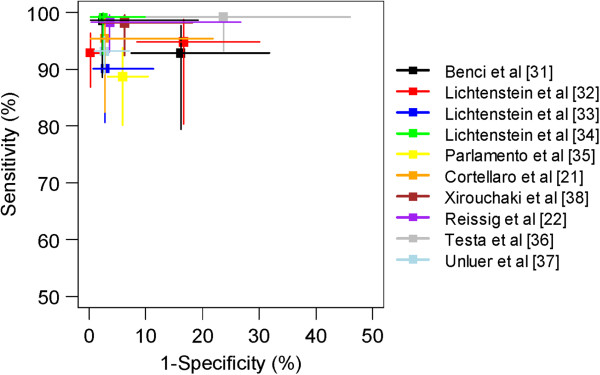
Results: Our initial search strategy yielded 2726 articles, of which 45 (1.7%) were manually selected for review and 10 (0.4%) were eligible for analyses. These 10 studies provided a combined sample size of 1172 participants. Six studies enrolled adult patients who were either hospitalized or admitted to Emergency Departments with suspicion of pneumonia and 4 studies enrolled critically-ill adult patients. LUS was performed by highly-skilled sonographers in seven studies, by trained physicians in two, and one did not mention level of training. All studies were conducted in high-income settings. LUS took a maximum of 13 minutes to conduct. Nine studies used a 3.5-5 MHz micro-convex transducer and one used a 5-9 MHz convex probe. Pooled sensitivity and specificity for the diagnosis of pneumonia using LUS were 94% (95% CI, 92%-96%) and 96% (94%-97%), respectively; pooled positive and negative LRs were 16.8 (7.7-37.0) and 0.07 (0.05-0.10), respectively; and, the area-under-the-ROC curve was 0.99 (0.98-0.99).
Conclusions: Our meta-analysis supports that LUS, when conducted by highly-skilled sonographers, performs well for the diagnosis of pneumonia. General practitioners and Emergency Medicine physicians should be encouraged to learn LUS since it appears to be an established diagnostic tool in the hands of experienced physicians.
Figures
Comment in
-
Thoracic ultrasound for the diagnosis of pneumonia in adults: a meta-analysis.Respir Res. 2015 Jul 25;16(1):89. doi: 10.1186/s12931-015-0248-9. Respir Res. 2015. PMID: 26205975 Free PMC article. No abstract available.
References
-
- Wiemken TL, Peyrani P, Ramirez JA. Global changes in the epidemiology of community-acquired pneumonia. Semin Respir Crit Care Med. 2012;33:213–219. - PubMed
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels DH, Basáñez MG, Baxter A, Bell ML, Benjamin EJ. et al.Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–2223. doi: 10.1016/S0140-6736(12)61689-4. - DOI - PubMed
-
- WHO. The top 10 causes of death 2013. 2013. Available from: http://www.who.int/mediacentre/factsheets/fs310/en/
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
