

Comparison of three techniques for ultrasound-guided femoral nerve catheter insertion: a randomized, blinded trial
- PMID: 24758775
- PMCID: PMC4110116
- DOI: 10.1097/ALN.0000000000000262
Comparison of three techniques for ultrasound-guided femoral nerve catheter insertion: a randomized, blinded trial
Abstract
Background: Ultrasound guidance for continuous femoral perineural catheters may be supplemented by electrical stimulation through a needle or through a stimulating catheter. The authors tested the primary hypothesis that ultrasound guidance alone is noninferior on both postoperative pain scores and opioid requirement and superior on at least one of the two. Second, the authors compared all interventions on insertion time and incremental cost.
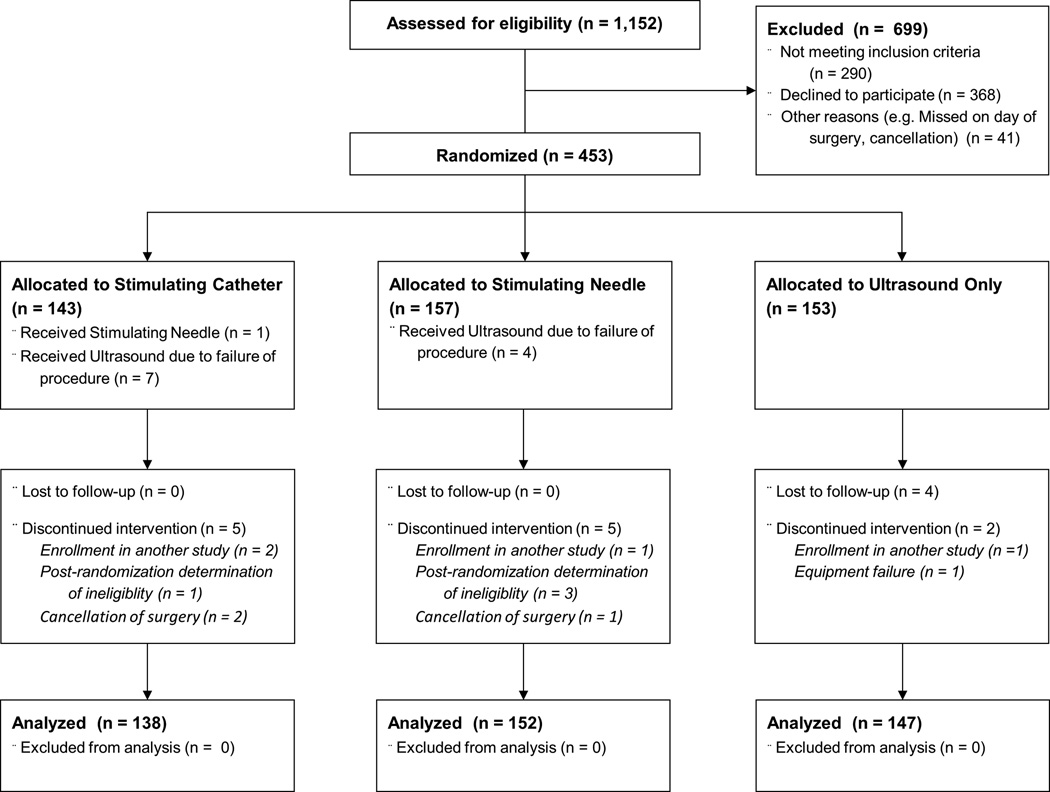
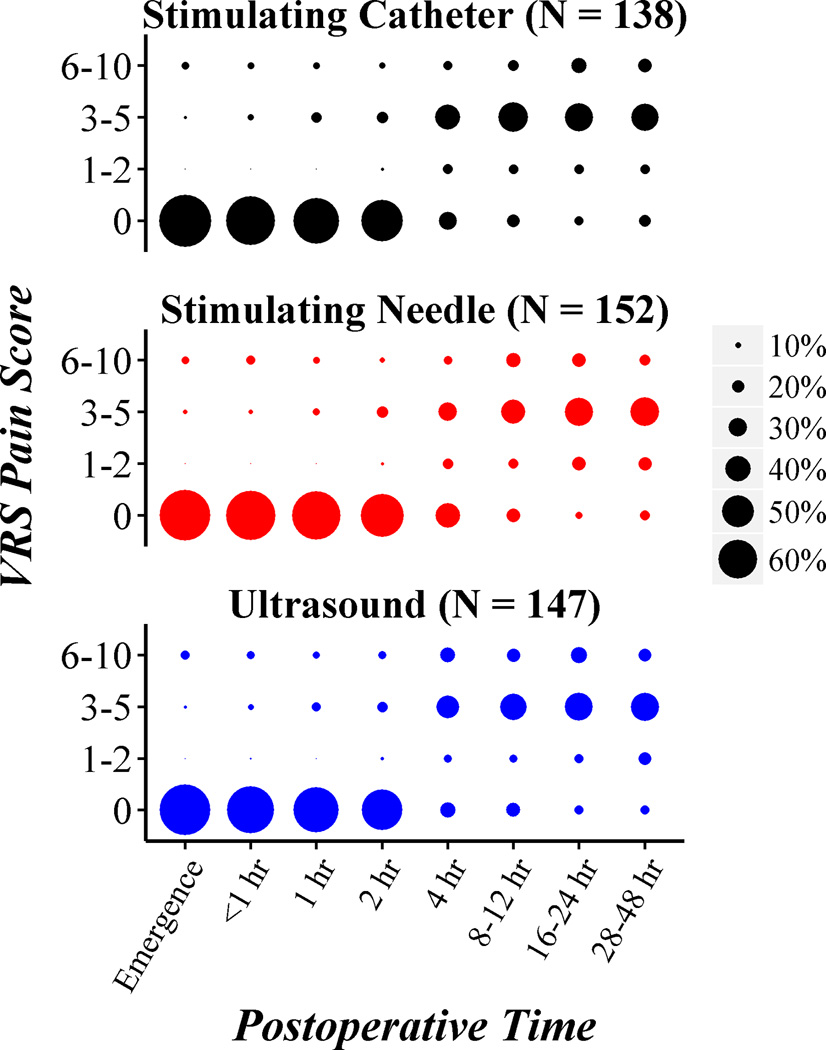
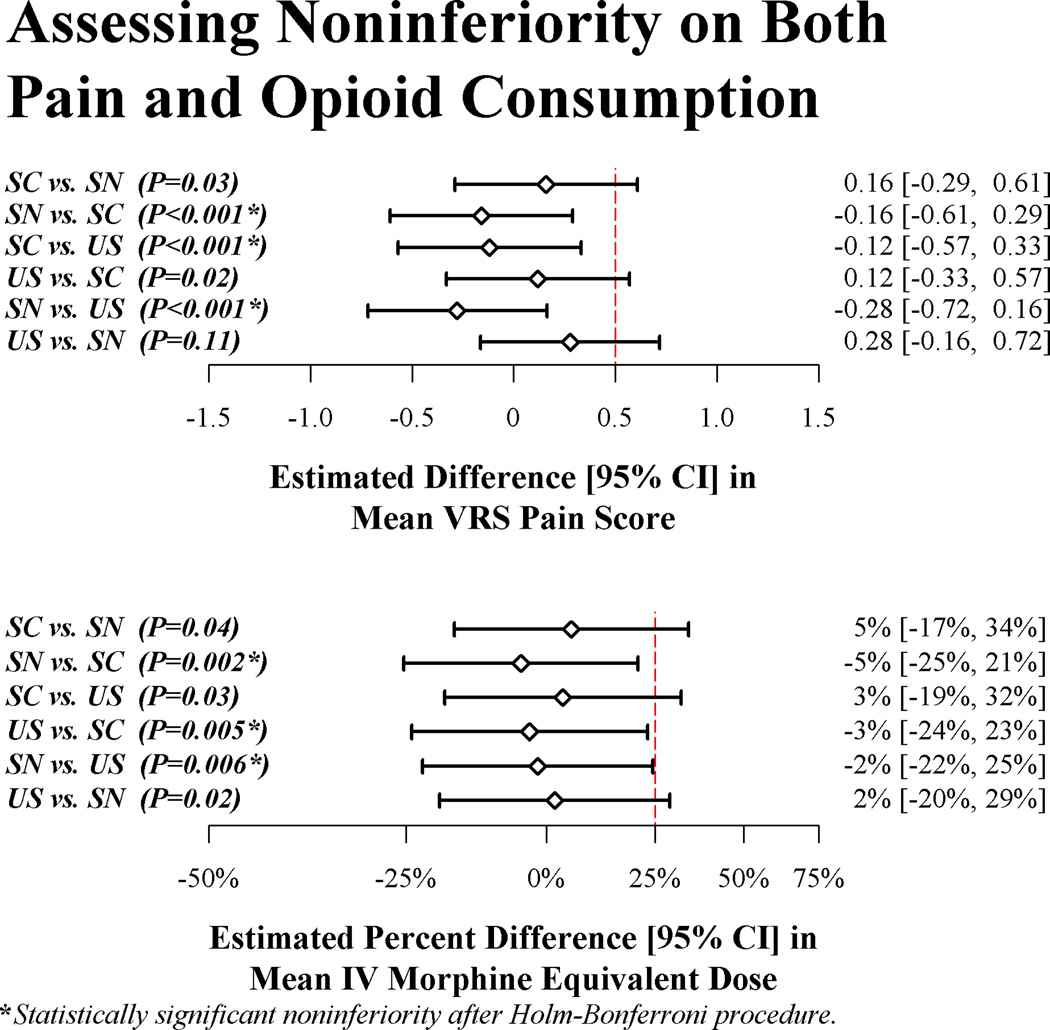
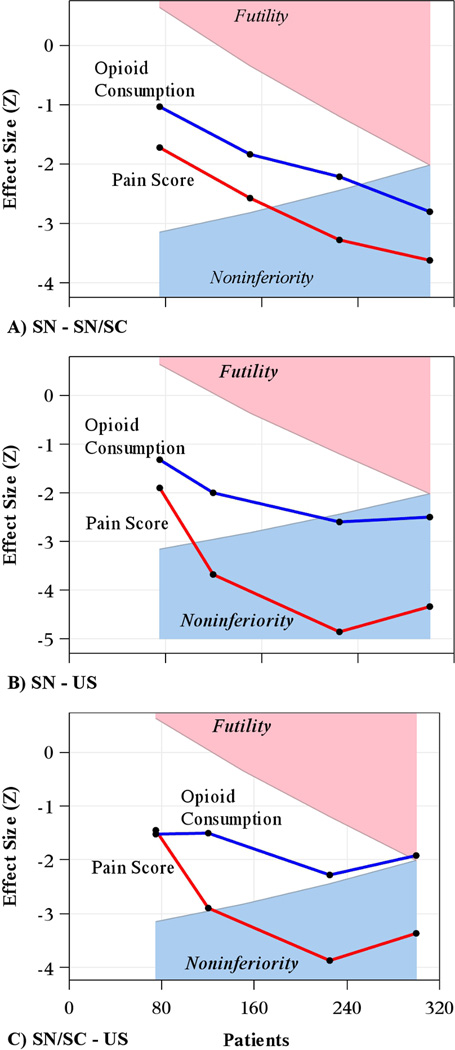
Methods: Patients having knee arthroplasty with femoral nerve catheters were randomly assigned to catheter insertion guided by: (1) ultrasound alone (n = 147); (2) ultrasound and electrical stimulation through the needle (n = 152); or (3) ultrasound and electrical stimulation through both the needle and catheter (n = 138). Noninferiority between any two interventions was defined for pain as not more than 0.5 points worse on a 0 to 10 verbal response scale and for opioid consumption as not more than 25% greater than the mean.
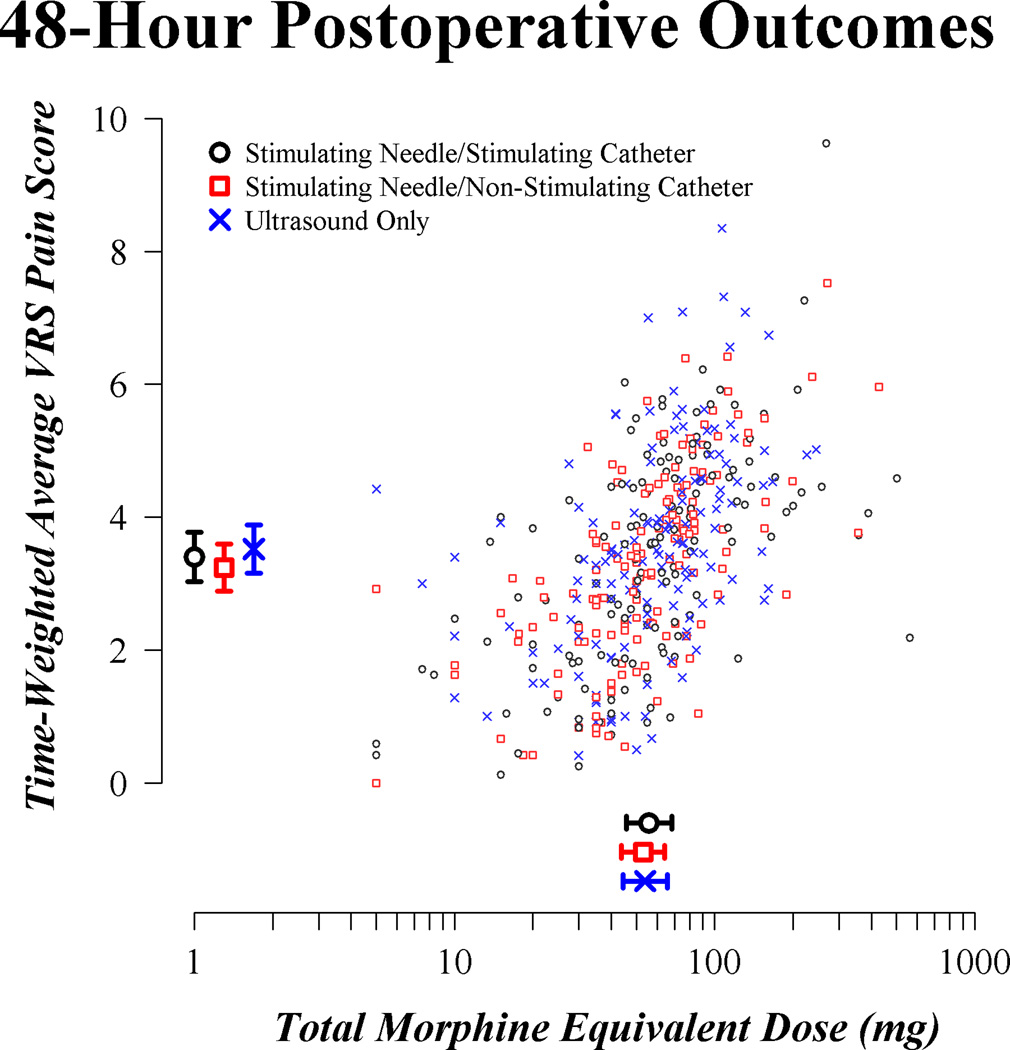
Results: The stimulating needle group was significantly noninferior to the stimulating catheter group (difference [95% CI] in mean verbal response scale pain score [stimulating needle vs. stimulating catheter] of -0.16 [-0.61 to 0.29], P < 0.001; percentage difference in mean IV morphine equivalent dose of -5% [-25 to 21%], P = 0.002) and to ultrasound-only group (difference in mean verbal response scale pain score of -0.28 [-0.72 to 0.16], P < 0.001; percentage difference in mean IV morphine equivalent dose of -2% [-22 to 25%], P = 0.006). In addition, the use of ultrasound alone for femoral nerve catheter insertion was faster and cheaper than the other two methods.
Conclusion: Ultrasound guidance alone without adding either stimulating needle or needle/catheter combination thus seems to be the best approach to femoral perineural catheters.
Figures
Comment in
-
When the statistics steal the show.Anesthesiology. 2015 Apr;122(4):952-3. doi: 10.1097/ALN.0000000000000590. Anesthesiology. 2015. PMID: 25782645 No abstract available.
-
Cost effectiveness of continuous femoral blocks for total knee replacement.Anesthesiology. 2015 Apr;122(4):953-4. doi: 10.1097/ALN.0000000000000591. Anesthesiology. 2015. PMID: 25782646 No abstract available.
-
In reply.Anesthesiology. 2015 Apr;122(4):954-5. doi: 10.1097/ALN.0000000000000592. Anesthesiology. 2015. PMID: 25782647 No abstract available.
References
-
- Morin A, Eberhart L, Behnke H, Wagner S, Koch T, Wolf U, Nau W, Kill C, Geldner G, Wulf H. Does femoral nerve catheter placement with stimulating catheters improve effective placement? A randomized, controlled, and observer-blinded trial. Anesth Analg. 2005;100:1503–1510. - PubMed
-
- Capdevila X, Barthelet Y, Biboulet P, Ryckwaert Y, Rubenovitch J, d'Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology. 1999;91:8–15. - PubMed
-
- Aveline C, Le Roux A, Le Hetet H, Vautier P, Cognet F, Bonnet F. Postoperative efficacies of femoral nerve catheters sited using ultrasound combined with neurostimulation compared with neurostimulation alone for total knee arthroplasty. Eur J Anaesthesiol. 2010;27:978–984. - PubMed
-
- Ilfeld BM, Le LT, Meyer RS, Mariano ER, Vandenborne K, Duncan PW, Sessler DI, Enneking FK, Shuster JJ, Theriaque DW, Berry LF, Spadoni EH, Gearen PF. Ambulatory continuous femoral nerve blocks decrease time to discharge readiness after tricompartment total knee arthroplasty: A randomized, triple-masked, placebo-controlled study. Anesthesiology. 2008;108:703–713. - PMC - PubMed
-
- Capdevila X, Biboulet P, Morau D, Bernard N, Deschodt J, Lopez S, d'Athis F. Continuous three-in-one block for postoperative pain after lower limb orthopedic surgery: Where do the catheters go? Anesth Analg. 2002;94:1001–1006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
