

doi: 10.1093/gastro/got005.
Epub 2013 Apr 4.
Total gastrectomy for locally advanced cancer: the pure laparoscopic approach
Affiliations
- PMID: 24759817
- PMCID: PMC3938005
- DOI: 10.1093/gastro/got005
Item in Clipboard
Total gastrectomy for locally advanced cancer: the pure laparoscopic approach
Gastroenterol Rep (Oxf).
2013 Sep.
No abstract available
Figures

(A) Placement of the trocars and position of the surgeons (1, 2 and 3). (B) Patient position and surgical set-up.

(A) The great omentum is sectioned 2 cm below the gastro-epiploic vessels to access to the omental cavity and to separate the gastric specimen from the omentum (group 4). (B, C) The right gastro-epiploic vein and artery are separately ligated at their origins (group 6).
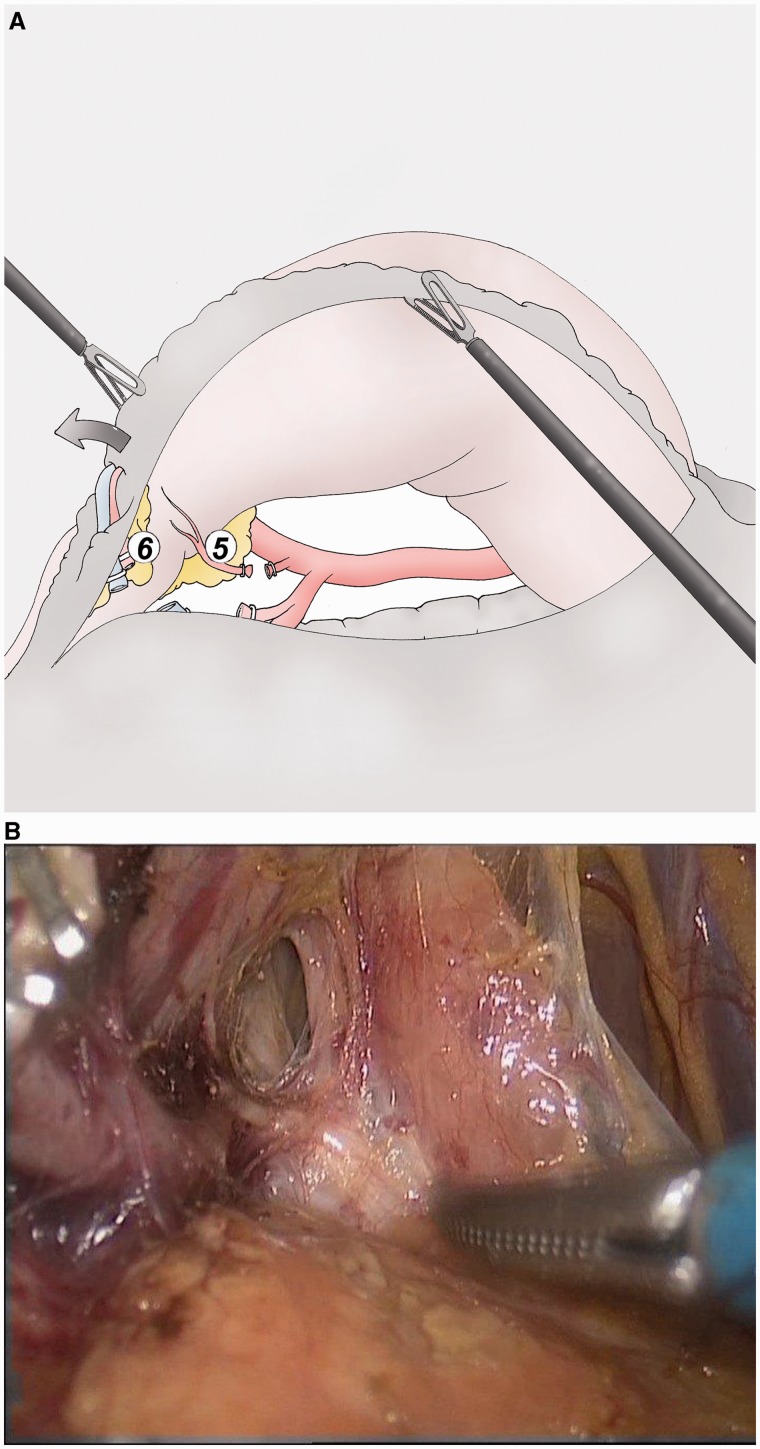
(A, B) The gastroduodenal artery is dissected along the posterior face of duodenum until its origin from the hepatic artery. The right gastric artery is then ligated (group 5).

(A) The lymphadenectomy of the group 8 is performed with the dissection of the common hepatic artery as far as the celiac trunk (group 9). The left gastric vein is sectioned to access to the left gastric artery and to cut it (group 7). The splenic artery is dissected for the first 3 cm. (B) Final aspect of the lymphadenectomy of the groups 7, 8 and 9. The right gastric artery is sectioned above standard clip, as well as the left gastric vein. The left gastric artery is sectioned above Hem-o-lock®.

(A) The dissection continues from back to the top along the aorta to the diaphragm and the oesophagus (groups 1 and 2). (B) The dissection rises up along the aorta to the diaphragm and the oesophagus (group 1).

(A) Section of the oesophagus 2 cm above the gastroesophageal junction using an Echelon Flex® 60 mm blue. (B) After the stapler section, the oesophagus lifts up in the mediastinum. A mild pressure using a Faucher tube maintains it in the abdomen.

(A) Separated lymphadenectomy of the group 12a (left part of the hepatic pedicle). (B) The left side of the hepatic pedicle is dissected along the hepatic artery and the portal vein (group 12A).

The great omentum is separately removed after the gastric resection using traction from left and right by the assistants.

Side-to-side jejunojejunostomy using an Echelon Flex® 60 mm blue.

The mesocolon is tracked by the assistants and opened above the ligament of Treitz. The alimentary loop is lifted up through this defect, which is then closed using a non-resorbable suture.

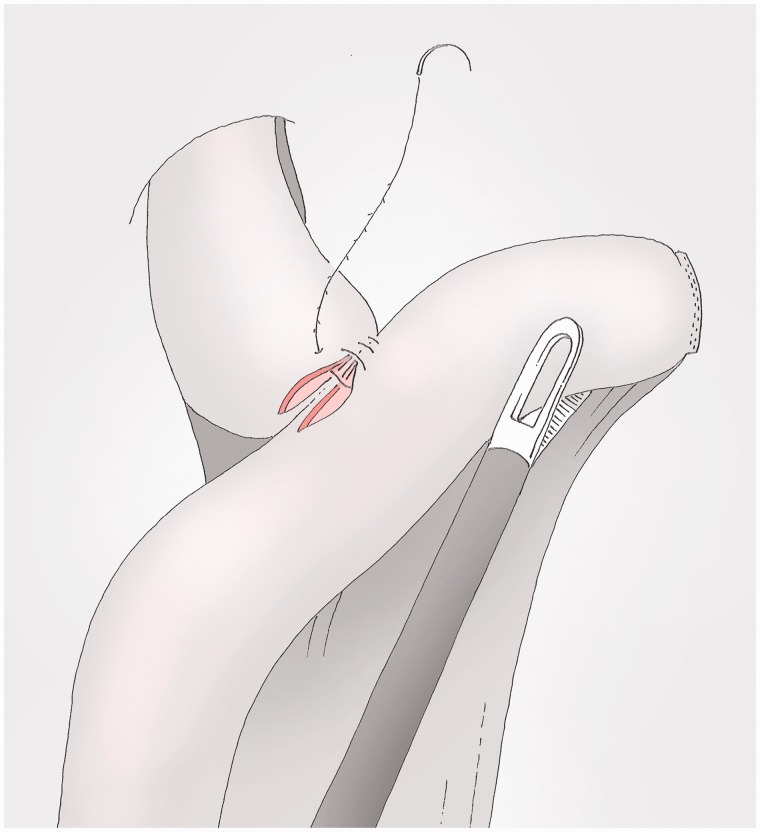
The oesophagus is maintained in the abdomen using a pressure on the Faucher tube and the jejunum is tracked to the left hypochondrium. The suture using a 15 cm V-loc® starts on the left and includes the oesophageal staple line.

The posterior side of the anastomosis is made by a full layer, manual, running suture; the wire is cut without knot with a 1.5 cm tail.

The viscera are opened, leaving a few millimetres at both extremities, with the help of a pressure on the Faucher tube for the oesophageal side.

Optional stitches of the posterior side of the anastomosis, using absorbable material in full layer fashion.
The anterior layer starts from the beginning of the posterior one and ends beyond the end of it. The wire is cut without knot with a 1.5 cm tail.

The alimentary loop is fixed to the pillar of the diaphragm.
References
-
- Azagra JS, Ibañez-Aguirre JF, Goergen M, et al. Long-term results of laparoscopic extended surgery in advanced gastric cancer: a series of 101 patients. Hepatogastroenterology. 2006;53:304–8. - PubMed
-
- Huang JL, Wei HB, Zheng ZH, et al. Laparoscopy-assisted D2 radical distal gastrectomy for advanced gastric cancer. Dig Surg. 2010;27:291–96. - PubMed
-
- Strong VE, Devaud N, Karpeh M. The role of laparoscopy for gastric surgery in the west. Review article. Gastric Cancer. 2009;12:127–31. - PubMed
-
- Nunobe S, Hiki N, Tanimura S, et al. Three-step esophagojejunal anastomosis with atraumatic anvil insertion technique after laparoscopic total gastrectomy. J Gastrointest Surg. 2011;15:1520–25. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
