

Value of transrectal ultrasonography for tumor node metastasis restaging in patients with locally advanced rectal cancer after neoadjuvant chemoradiotherapy
- PMID: 24759964
- PMCID: PMC3937995
- DOI: 10.1093/gastro/got028
Value of transrectal ultrasonography for tumor node metastasis restaging in patients with locally advanced rectal cancer after neoadjuvant chemoradiotherapy
Abstract
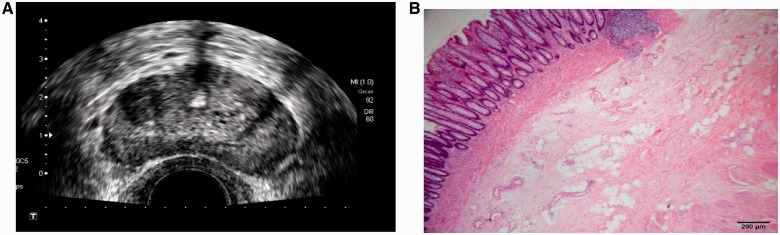
Objective: To explore the value of transrectal ultrasonography (TRUS) for tumor node metastasis (TNM) restaging for patients with locally advanced rectal cancer after neoadjuvant chemoradiotherapy (neo-CRT).
Methods: One hundred and forty-nine patients with locally advanced rectal cancer (cT3-4 or cN+) who underwent TRUS after neo-CRT were retrospectively reviewed. TRUS restaging was compared with the results of post-operative pathological TNM findings.
Results: After neo-CRT, the accuracy of TRUS for diagnosing T-staging was 30.9%, with 60.4% (90/149) of cases overestimated. The sensitivity of TRUS for T-staging (T0 vs T1 vs T2 vs T3 vs T4) were 16.3%, 0%, 12.5%, 42.6% and 75.0%, respectively. The accuracy of TRUS for diagnosing N-staging after neo-CRT was 81.2%, with the sensitivities of N0 and N+ were 93.3% and 31.0%, respectively. After neo-CRT, 27.5% (41/149) of patients achieved pathologically complete response (pCR). The sensitivity, specificity, positive predictive value and negative predictive values of TRUS for pCR were 17.1%, 99.1%, 87.5% and 75.9%, respectively.
Conclusions: TRUS can be applied for restaging T4 and N0, and has potential for screening out patients with pCR in those with locally advanced rectal cancer after neo-CRT, although some stages are overestimated for T-staging and its sensitivity for predicting pCR is low.
Keywords: Rectal cancer; TNM restaging; neo-chemoradiotherapy (neo-CRT); transrectal ultrasonography (TRUS).
Figures


Similar articles
-
Application value of biplane transrectal ultrasonography plus ultrasonic elastosonography and contrast-enhanced ultrasonography in preoperative T staging after neoadjuvant chemoradiotherapy for rectal cancer.Eur J Radiol. 2018 Jul;104:20-25. doi: 10.1016/j.ejrad.2018.04.027. Epub 2018 Apr 27. Eur J Radiol. 2018. PMID: 29857861
-
Accuracy of transrectal ultrasound after preoperative radiochemotherapy compared to computed tomography and magnetic resonance in locally advanced rectal cancer.Int J Colorectal Dis. 2012 Jul;27(7):967-73. doi: 10.1007/s00384-012-1419-5. Epub 2012 Feb 3. Int J Colorectal Dis. 2012. PMID: 22297865
-
The potential of restaging in the prediction of pathologic response after preoperative chemoradiotherapy for rectal cancer.Ann Surg Oncol. 2007 Feb;14(2):455-61. doi: 10.1245/s10434-006-9269-4. Epub 2006 Dec 2. Ann Surg Oncol. 2007. PMID: 17139456
-
Accuracy of Endorectal Endoscopic Ultrasound (EUS) for Locally Advanced Rectal Cancer (LARC) Restaging After Neoadjuvant Chemoradiotherapy (NAT): A Meta-Analysis.Hepatogastroenterology. 2014 Jun;61(132):978-83. Hepatogastroenterology. 2014. PMID: 26158152 Review.
-
Diagnostic Value of Endoscopic Ultrasound after Neoadjuvant Chemotherapy for Gastric Cancer Restaging: A Meta-Analysis of Diagnostic Test.Diagnostics (Basel). 2022 Jan 3;12(1):100. doi: 10.3390/diagnostics12010100. Diagnostics (Basel). 2022. PMID: 35054266 Free PMC article. Review.
Cited by
-
Predictive value of APAF-1 and COX-2 expression in pathologic complete response to neoadjuvant chemoradiotherapy for patients with locally advanced rectal adenocarcinoma.Oncotarget. 2016 Jun 7;7(23):35233-40. doi: 10.18632/oncotarget.9125. Oncotarget. 2016. PMID: 27153549 Free PMC article.
References
-
- Sauer R, Becker H, Hohenberger W, et al. Pre-operative versus post-operative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351:1731–40. - PubMed
-
- Bosset JF, Collette L, Calais G, et al. Chemotherapy with pre-operative radiotherapy in rectal cancer. N Engl J Med. 2006;355:1114–23. - PubMed
-
- Martin ST, Heneghan HM, Winter DC. Systematic review and meta-analysis of outcomes following pathological complete response to neoadjuvant chemoradiotherapy for rectal cancer. Br J Surg. 2012;99:918–28. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
