

Elevated double negative T cells in pediatric autoimmunity
- PMID: 24760111
- PMCID: PMC4047151
- DOI: 10.1007/s10875-014-0038-z
Elevated double negative T cells in pediatric autoimmunity
Abstract
Purpose: Autoimmune diseases are thought to be caused by a loss of self-tolerance of the immune system. One candidate marker of immune dysregulation in autoimmune disease is the presence of increased double negative T cells (DNTs) in the periphery. DNTs are characteristically elevated in autoimmune lymphoproliferative syndrome, a systemic autoimmune disease caused by defective lymphocyte apoptosis due to Fas pathway defects. DNTs have also been found in the peripheral blood of adult patients with systemic lupus erythematosus (SLE), where they may be pathogenic. DNTs in children with autoimmune disease have not been investigated.
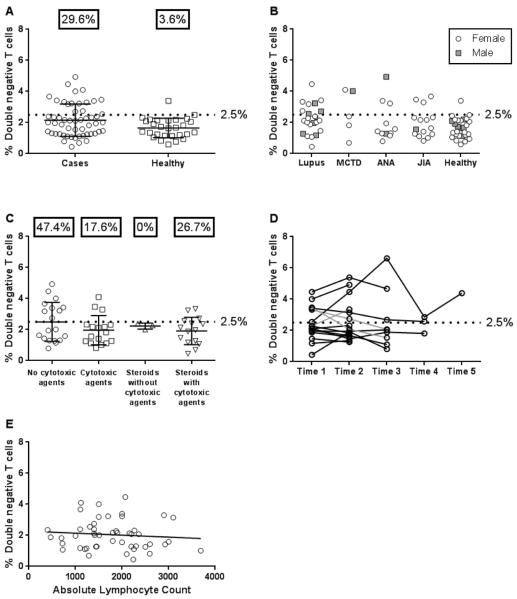
Methods: We evaluated DNTs in pediatric patients with SLE, mixed connective tissue disease (MCTD), juvenile idiopathic arthritis (JIA), or elevated antinuclear antibody (ANA) but no systemic disease. DNTs (CD3(+)CD56(-)TCRαβ(+)CD4(-)CD8(-)) from peripheral blood mononuclear cells were analyzed by flow cytometry from 54 pediatric patients including: 23 SLE, 15 JIA, 11 ANA and 5 MCTD compared to 28 healthy controls.
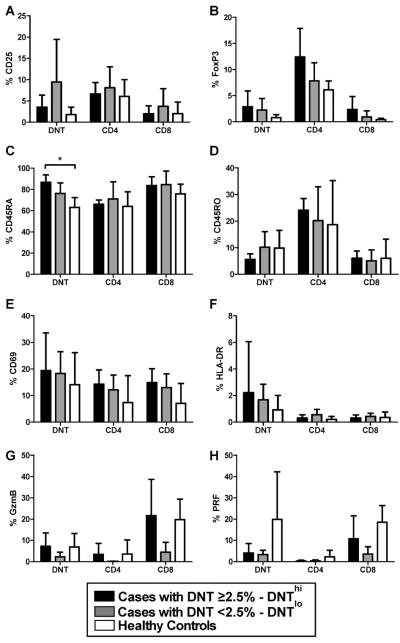
Results: Sixteen cases (29.6 %) had elevated DNTs (≥2.5 % of CD3(+)CD56(-)TCRαβ(+) cells) compared to 1 (3.6 %) control. Medication usage including cytotoxic drugs and absolute lymphocyte count were not associated with DNT levels, and percentages of DNTs were stable over time. Analysis of multiple phenotypic and activation markers showed increased CD45RA expression on DNTs from patients with autoimmune disease compared to controls.
Conclusion: DNTs are elevated in a subset of pediatric patients with autoimmune disease and additional investigations are required to determine their precise role in autoimmunity.
Figures
Similar articles
-
T-regs in autoimmune hepatitis-systemic lupus erythematosus/mixed connective tissue disease overlap syndrome are functionally defective and display a Th1 cytokine profile.J Autoimmun. 2013 Mar;41:146-51. doi: 10.1016/j.jaut.2012.12.003. Epub 2013 Jan 1. J Autoimmun. 2013. PMID: 23287048
-
Peripheral blood lymphocytes in SLE--hyperexpression of CD154 on T and B lymphocytes and increased number of double negative T cells.J Autoimmun. 1998 Oct;11(5):471-5. doi: 10.1006/jaut.1998.0213. J Autoimmun. 1998. PMID: 9802931
-
Targeting Notch signaling in autoimmune and lymphoproliferative disease.Blood. 2008 Jan 15;111(2):705-14. doi: 10.1182/blood-2007-05-087353. Epub 2007 Oct 9. Blood. 2008. PMID: 17925488 Free PMC article.
-
Clinical utility of antinuclear antibody tests in children.BMC Pediatr. 2004 Jul 9;4:13. doi: 10.1186/1471-2431-4-13. BMC Pediatr. 2004. PMID: 15245579 Free PMC article. Review.
-
TCRαβ+CD3+CD4-CD8- (double negative) T cells in autoimmunity.Autoimmun Rev. 2018 Apr;17(4):422-430. doi: 10.1016/j.autrev.2018.02.001. Epub 2018 Feb 9. Autoimmun Rev. 2018. PMID: 29428806 Review.
Cited by
-
The Potential of Harnessing IL-2-Mediated Immunosuppression to Prevent Pathogenic B Cell Responses.Front Immunol. 2021 Apr 27;12:667342. doi: 10.3389/fimmu.2021.667342. eCollection 2021. Front Immunol. 2021. PMID: 33986755 Free PMC article. Review.
-
Age-Related Differences in Percentages of Regulatory and Effector T Lymphocytes and Their Subsets in Healthy Individuals and Characteristic STAT1/STAT5 Signalling Response in Helper T Lymphocytes.J Immunol Res. 2015;2015:352934. doi: 10.1155/2015/352934. Epub 2015 Oct 7. J Immunol Res. 2015. PMID: 26525134 Free PMC article.
-
Associations of Lymphocyte Subpopulations, Related Cytokines, Clinical Phenotypes, and Outcomes in Systemic Juvenile Idiopathic Arthritis.ACR Open Rheumatol. 2025 Aug;7(8):e70070. doi: 10.1002/acr2.70070. ACR Open Rheumatol. 2025. PMID: 40728052 Free PMC article.
-
Double negative T cells, a potential biomarker for systemic lupus erythematosus.Precis Clin Med. 2020 Mar;3(1):34-43. doi: 10.1093/pcmedi/pbaa001. Epub 2020 Jan 20. Precis Clin Med. 2020. PMID: 32257532 Free PMC article.
-
Flow Cytometry Contributions for the Diagnosis and Immunopathological Characterization of Primary Immunodeficiency Diseases With Immune Dysregulation.Front Immunol. 2019 Nov 26;10:2742. doi: 10.3389/fimmu.2019.02742. eCollection 2019. Front Immunol. 2019. PMID: 31849949 Free PMC article. Review.
References
-
- Thomas JW. Antigen-specific responses in autoimmunity and tolerance. Immunol Res. 2001;23:235–44. - PubMed
-
- Sieling PA, Porcelli SA, Duong BT, Spada F, Bloom BR, Diamond B, et al. Human double-negative T cells in systemic lupus erythematosus provide help for IgG and are restricted by CD1c. J Immunol. 2000;165:5338–44. - PubMed
-
- Fleisher TA, Oliveira JB. Monogenic defects in lymphocyte apoptosis. Curr Opin Allergy Clin Immunol. 2012;12:609–15. - PubMed
-
- Vaishnaw AK, Toubi E, Ohsako S, Drappa J, Buys S, Estrada J, et al. The spectrum of apoptotic defects and clinical manifestations, including systemic lupus erythematosus, in humans with CD95 (Fas/APO-1) mutations. Arthritis Rheum. 1999;42:1833–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
