

Neoadjuvant therapy followed by local excision and two-stage total mesorectal excision: a new strategy for sphincter preservation in locally advanced ultra-low rectal cancer
- PMID: 24760235
- PMCID: PMC3920994
- DOI: 10.1093/gastro/got040
Neoadjuvant therapy followed by local excision and two-stage total mesorectal excision: a new strategy for sphincter preservation in locally advanced ultra-low rectal cancer
Abstract
Background: With the increased usage of neoadjuvant chemoradiotherapy, improved surgical technique and stapling devices, sphincter-preserving resection has become more frequent for patients with rectal cancer. However, as for locally advanced ultra-low rectal cancer, sphincter-preservation is still facing an enormous challenge.
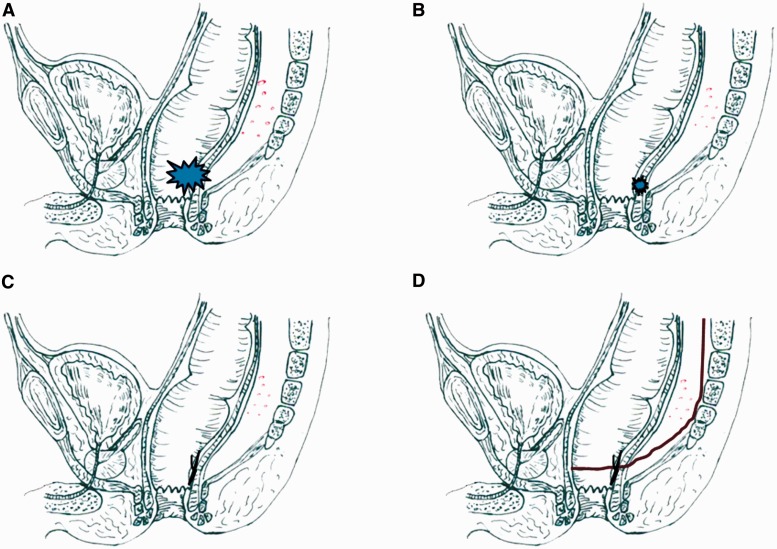
Objective: To introduce an NLT strategy of sphincter-preservation-neoadjuvant therapy (NT) followed by local excision (LE) and two-stage total mesorectal excision (TME)-into the treatment of locally advanced ultra-low rectal cancer (lesions with anal sphincter invasion).
Methods: From October 2010 to October 2011, nine patients with locally advanced rectal cancer located less than 3 cm from the anal verge were treated by the NLT strategy. All patients had shown good clinical response to NT. The LE procedure was carried transanally 6-8 weeks after completion of the NT. TME was performed to dissect mesorectal lymph nodes 4-6 weeks after LE.
Results: Of the nine patients, the lesion was assessed as T2 in two, T3 in five, and T4 in two before NT, and lymph node metastasis was detected in five patients. The median distance from the tumor to the anal verge was 2.5 cm (range: 1-3 cm). The median follow-up was 27 months (range: 24-34 months). No distant metastasis was detected. Only one patient (11.1%) developed local recurrence at 12 months post-operatively and then underwent abdomino-perineal resection. The remaining eight patients had preserved long-term continence and the median Wexner score at two years post-operation was 4 (range: 2-6).
Conclusion: The new NLT strategy can achieve sphincter-preservation in some patients with ultra-low rectal cancer, with favorable oncological outcome and preservation of normal anal sphincter function.
Keywords: rectal cancer; sphincter-preservation; neoadjuvant therapy; local excision; total mesorectal excision.
Figures

References
-
- van Gijn W, Marijnen CA, Nagtegaal ID, et al. Dutch Colorectal Cancer Group. Pre-operative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011;12:575–82. - PubMed
-
- Valentini V, Aristei C, Glimelius B, et al. Scientific Committee. Multidisciplinary rectal cancer management: 2nd European rectal cancer consensus conference (EURECAcc2) Radiother Oncol. 2009;92:148–63. - PubMed
-
- Williams NS, Dixon MF, Johnston D. Reappraisal of the 5 centimetre rule of distal excision for carcinoma of the rectum: a study of distal intramural spread and of patients’ survival. Br J Surg. 1983;70:150–54. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
