

Universal newborn screening for congenital CMV infection: what is the evidence of potential benefit?
- PMID: 24760655
- PMCID: PMC4494732
- DOI: 10.1002/rmv.1790
Universal newborn screening for congenital CMV infection: what is the evidence of potential benefit?
Abstract
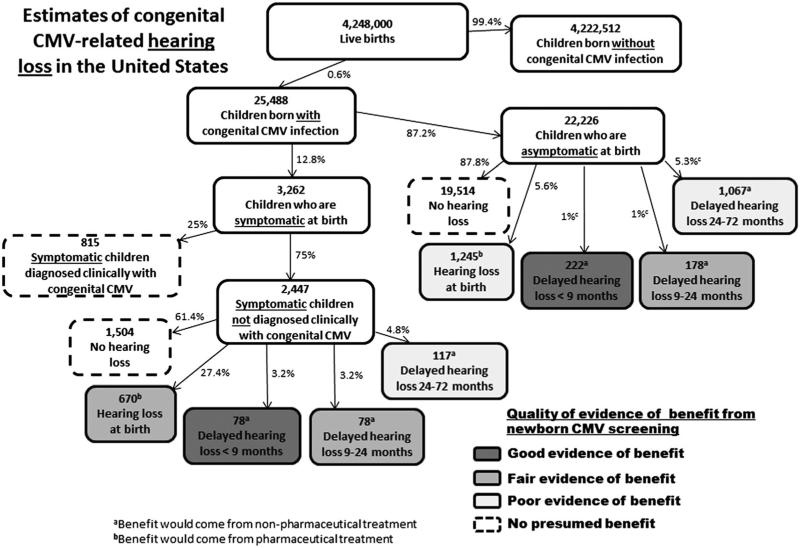
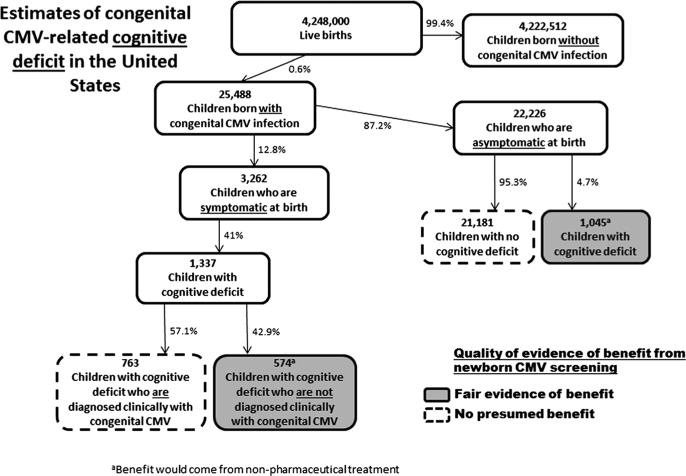
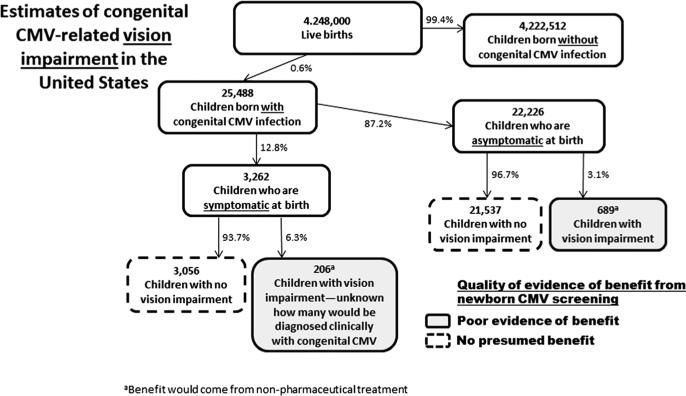
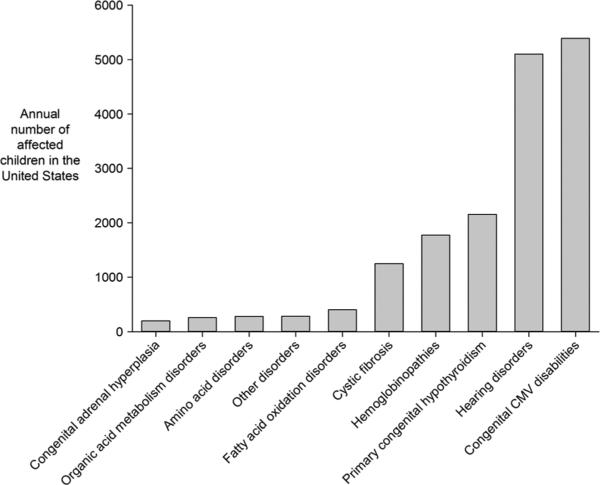
Congenital CMV infection is a leading cause of childhood disability. Many children born with congenital CMV infection are asymptomatic or have nonspecific symptoms and therefore are typically not diagnosed. A strategy of newborn CMV screening could allow for early detection and intervention to improve clinical outcomes. Interventions might include antiviral drugs or nonpharmaceutical therapies such as speech-language therapy or cochlear implants. Using published data from developed countries, we analyzed existing evidence of potential benefit that could result from newborn CMV screening. We first estimated the numbers of children with the most important CMV-related disabilities (i.e. hearing loss, cognitive deficit, and vision impairment), including the age at which the disabilities occur. Then, for each of the disabilities, we examined the existing evidence for the effectiveness of various interventions. We concluded that there is good evidence of potential benefit from nonpharmaceutical interventions for children with delayed hearing loss that occurs by 9 months of age. Similarly, we concluded that there is fair evidence of potential benefit from antiviral therapy for children with hearing loss at birth and from nonpharmaceutical interventions for children with delayed hearing loss occurring between 9 and 24 months of age and for children with CMV-related cognitive deficits. We found poor evidence of potential benefit for children with delayed hearing loss occurring after 24 months of age and for children with vision impairment. Overall, we estimated that in the United States, several thousand children with congenital CMV could benefit each year from newborn CMV screening, early detection, and interventions.
Copyright © 2014 John Wiley & Sons, Ltd.
Figures
References
-
- Griffiths PD, Walter S. Cytomegalovirus. Current Opinion in Infectious Diseases. 2005;18:241–245. - PubMed
-
- McMullan BJ, Palasanthiran P, Jones CA, et al. Congenital cytomegalovirus—time to diagnosis, management and clinical sequelae in Australia: opportunities for earlier identification. Medical Journal of Australia. 2011;194:625–629. - PubMed
-
- Cannon MJ. Congenital cytomegalovirus (CMV) epidemiology and awareness. Journal of Clinical Virology. 2009;46S:S6–S10. - PubMed
-
- Institute of Medicine Committee to Study Priorities for Vaccine D . Vaccines for the 21st Century: A Tool for Decision Making. National Academy Press; Washington D. C.: 2000.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
