

Outcomes of fluoroscopically guided lumbar transforaminal epidural steroid injections in degenerative lumbar spondylolisthesis patients
- PMID: 24761192
- PMCID: PMC3996334
- DOI: 10.4184/asj.2014.8.2.119
Outcomes of fluoroscopically guided lumbar transforaminal epidural steroid injections in degenerative lumbar spondylolisthesis patients
Abstract
Study design: A prospective cohort.
Purpose: To report the short and long term outcomes of fluoroscopically guided lumbar transforaminal epidural steroid injection (TFESI) in degenerative lumbar spondylolisthesis (DLS) patients.
Overview of literature: TFESI has been widely used for the treatment of lumbosacral radicular pains. However, to our knowledge, there has been no study which has evaluated the outcomes of TFESI in patients with DLS.
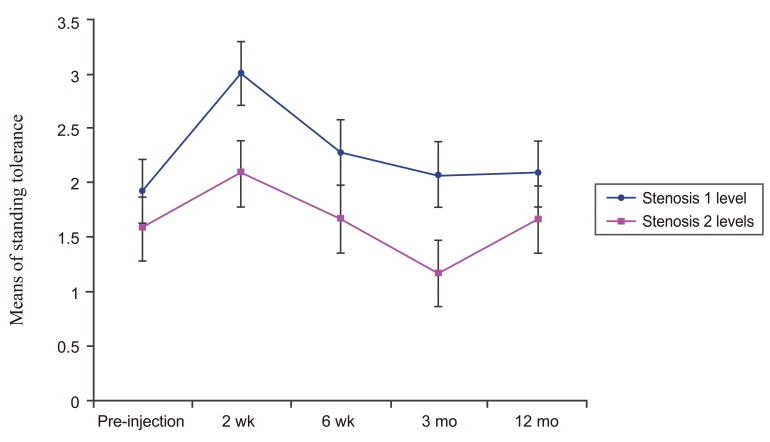
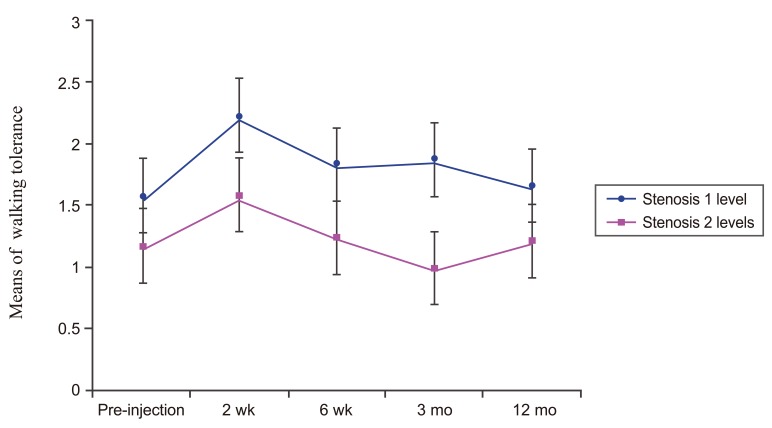
Methods: The DLS patients received fluoroscopically guided lumbar TFESI with 80 mg of methylprednisolone and 2 mL of 1% lidocaine hydrochloride. Patients were evaluated by an independent observer before the initial injection, at 2 weeks, at 6 weeks, at 3 months, and at 12 months after the injections. Visual analog scale (VAS), Roland 5-point pain scale, standing tolerance, walking tolerance, and patient satisfaction scale were evaluated for outcomes.
Results: Thirty three DLS patients treated with TFESI, who were completely followed up, were included in this study. The average number of injections per patient was 1.9 (range from 1 to 3 injections per patient). Significant improvements in VAS and Roland 5-point pain scale were observed over the follow up period from 2 weeks to 12 months. However, the standing and walking tolerance were not significantly improved after 2 weeks. At 2 weeks, the patient satisfaction scale was highest, although, these outcomes declined with time. The DLS patients with one level of spinal stenosis showed significantly better outcome than the DLS patients with two levels of spinal stenosis. Five patients (13%) underwent surgical treatment during the 3 to 12 months follow up.
Conclusions: TFESI provides short term improvements in VAS and Roland 5-point pain scale, standing tolerance, walking tolerance and patient satisfaction scale in DLS patients. In the long term, it improves VAS but limits the improvements in Roland 5-point pain scale, standing tolerance, walking tolerance and patient satisfaction scale.
Keywords: Degenerative lumbar; Epidural injection; Outcome; Spondylolisthesis; Steroid.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures




References
-
- Vibert BT, Sliva CD, Herkowitz HN. Treatment of instability and spondylolisthesis: surgical versus nonsurgical treatment. Clin Orthop Relat Res. 2006;443:222–227. - PubMed
-
- Lutz GE, Vad VB, Wisneski RJ. Fluoroscopic transforaminal lumbar epidural steroids: an outcome study. Arch Phys Med Rehabil. 1998;79:1362–1366. - PubMed
-
- Weinstein SM, Herring SA, Derby R. Contemporary concepts in spine care. Epidural steroid injections. Spine (Phila Pa 1976) 1995;20:1842–1846. - PubMed
-
- Stewart HD, Quinnell RC, Dann N. Epidurography in the management of sciatica. Br J Rheumatol. 1987;26:424–429. - PubMed
-
- Abdi S, Datta S, Lucas LF. Role of epidural steroids in the management of chronic spinal pain: a systematic review of effectiveness and complications. Pain Physician. 2005;8:127–143. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
