

A Preliminary Study on the Effects of Self-Reported Dietary Caffeine on Pain Experience and Postoperative Analgesia
- PMID: 24761271
- PMCID: PMC3621341
- DOI: 10.1089/jcr.2012.0016
A Preliminary Study on the Effects of Self-Reported Dietary Caffeine on Pain Experience and Postoperative Analgesia
Abstract
Background: Caffeine reduces the amount of analgesic medications necessary to provide postoperative pain (POP) relief and augments treatments for headaches and dental pain. Despite considerable evidence of its beneficial effects, little is understood about the role of dietary caffeine consumption on baseline pain sensitivity or POP following oral surgery.
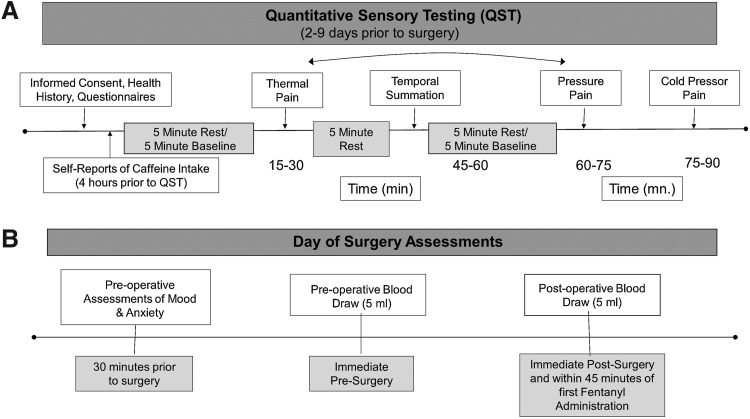
Method: Baseline experimental pain testing (quantitative sensory testing [QST]) using four stimulus modalities was conducted on 30 healthy adults (53% females) before surgical extraction of four third molars. Self-reported caffeine ingestion was reported before QST, and on the day of surgery, preoperative and postoperative caffeine plasma concentrations (CPC) were measured by mass spectrometry. POP ratings were obtained at timed intervals.
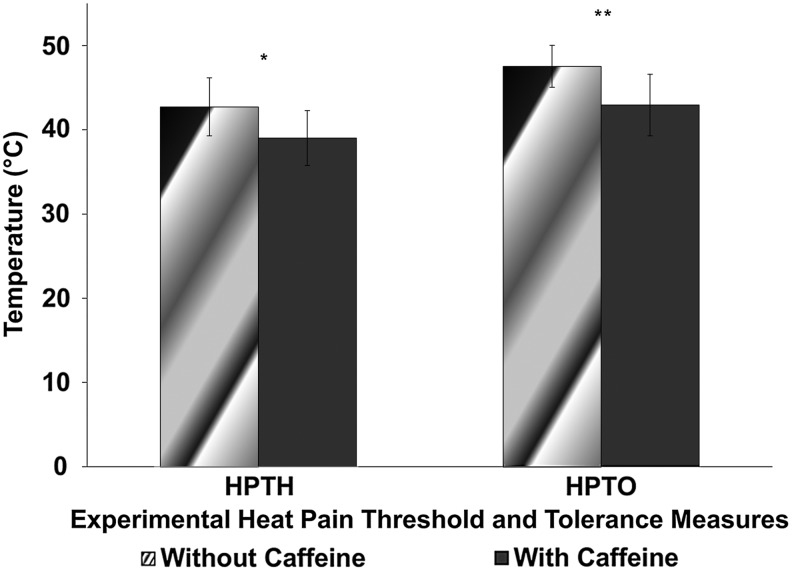
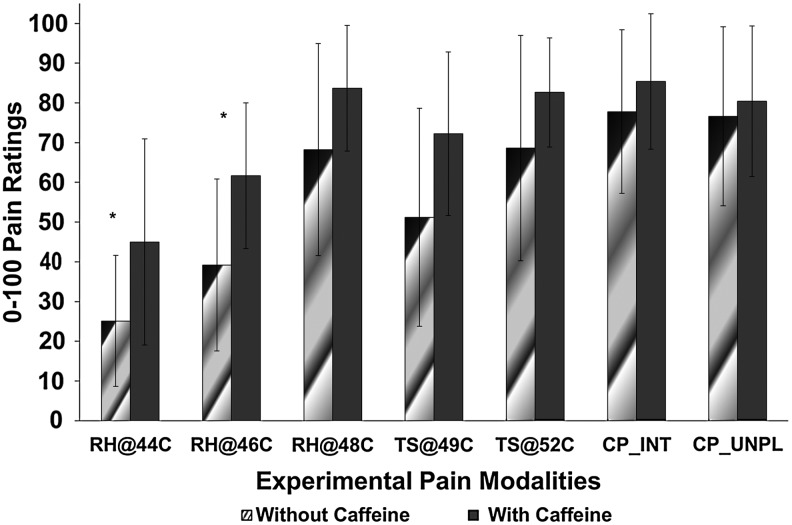
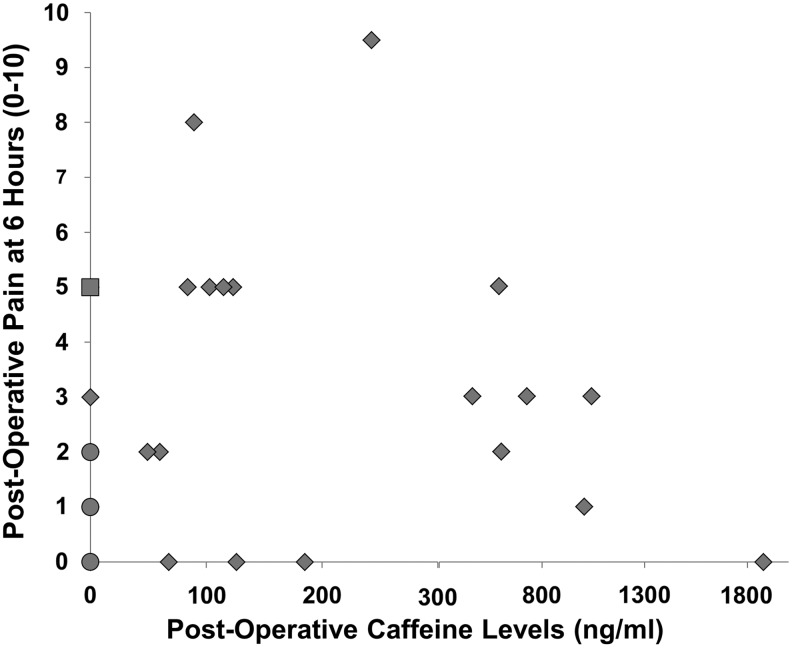
Results: In QST, compared to subjects who self-reported no caffeine intake, those who self-reported caffeine ingestion demonstrated a higher pain sensitivity, particularly, on ramp and hold sustained heat at 44°C and 46°C, as well as a lower heat pain threshold and tolerance (p=0.05). Differences approached significance (p=0.06) in POP between subjects with CPC above 300 ng/mL and those with CPC below 300 ng/mL. Specifically, those with >300 ng/mL CPC had a slightly lower POP (mean 2.43, range 0-5) compared to those with <300 ng/mL CPC whose POP ratings were slightly higher (mean 2.89) with a greater variability (range 0-9.5).
Conclusions: Self-reported, dietary caffeine intake was associated with higher QST ratings with lower threshold and tolerance particularly on heat pain modalities. External factors (i.e., analgesic dosage) may have played a role in the analgesic effects of caffeine on POP in oral surgery, especially in individuals with CPC exceeding 300 ng/mL who reported lower pain.
Figures
References
-
- Sawynok J. Caffeine and pain. Pain. 2011;152:726–729. - PubMed
-
- Derry CJ. Derry S. Moore RA. Caffeine as an analgesic adjuvant for acute pain in adults. Cochrane Database Syst Rev. 2012;3 CD009281.:CD009281. - PubMed
-
- Sawynok J. Methylxanthines and pain. Handb Exp Pharmacol. 2011;200:311–329. - PubMed
-
- Werner MU. Mjobo HN. Nielsen PR. Rudin A. Prediction of postoperative pain: a systematic review of predictive experimental pain studies. Anesthesiology. 2010;112:1494–1502. - PubMed
-
- Staahl C. Drewes AM. Experimental human pain models: a review of standardised methods for preclinical testing of analgesics. Basic Clin Pharmacol Toxicol. 2004;95:97–111. - PubMed
LinkOut - more resources
Full Text Sources