

Using an Agent-Based Model to Examine the Role of Dynamic Bacterial Virulence Potential in the Pathogenesis of Surgical Site Infection
- PMID: 24761337
- PMCID: PMC3842882
- DOI: 10.1089/wound.2012.0400
Using an Agent-Based Model to Examine the Role of Dynamic Bacterial Virulence Potential in the Pathogenesis of Surgical Site Infection
Abstract
Objective: Despite clinical advances, surgical site infections (SSIs) remain a problem. The development of SSIs involves a complex interplay between the cellular and molecular mechanisms of wound healing and contaminating bacteria, and here, we utilize an agent-based model (ABM) to investigate the role of bacterial virulence potential in the pathogenesis of SSI.
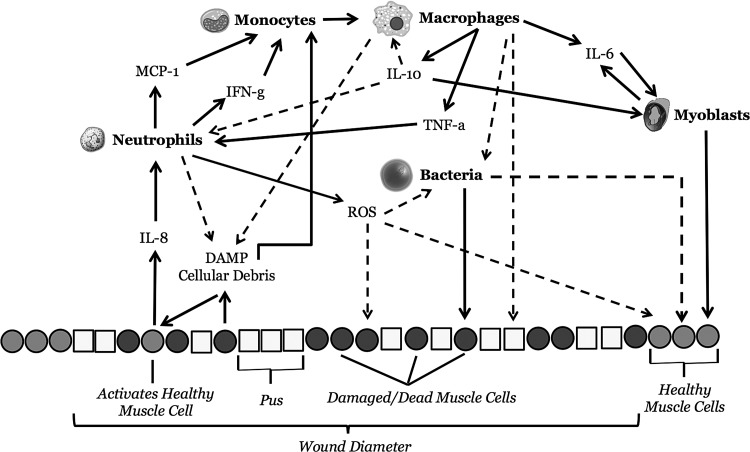
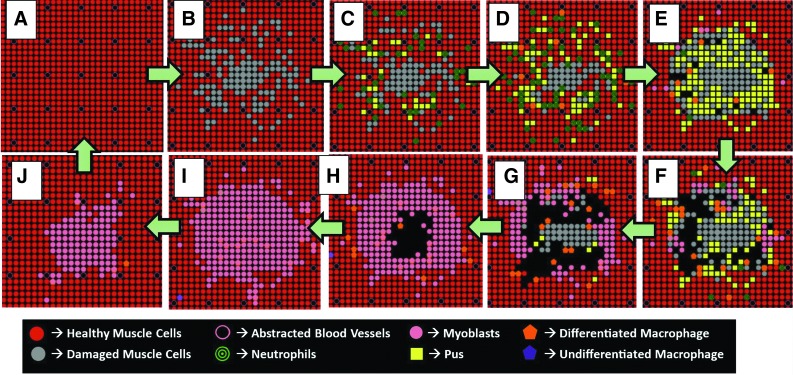
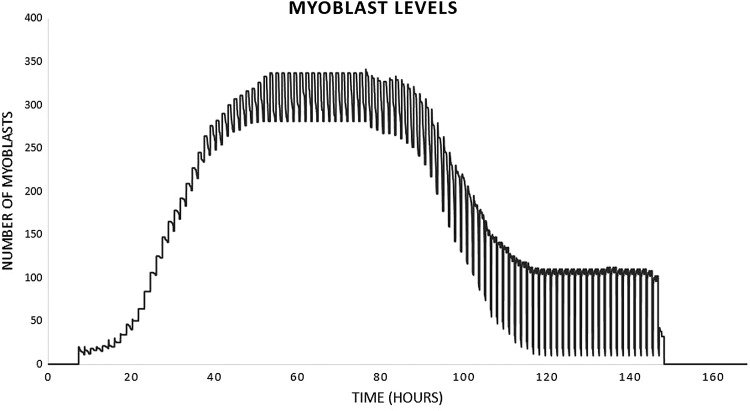
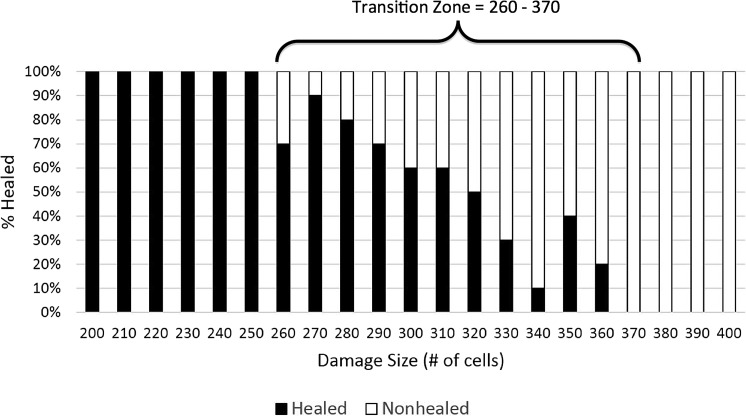
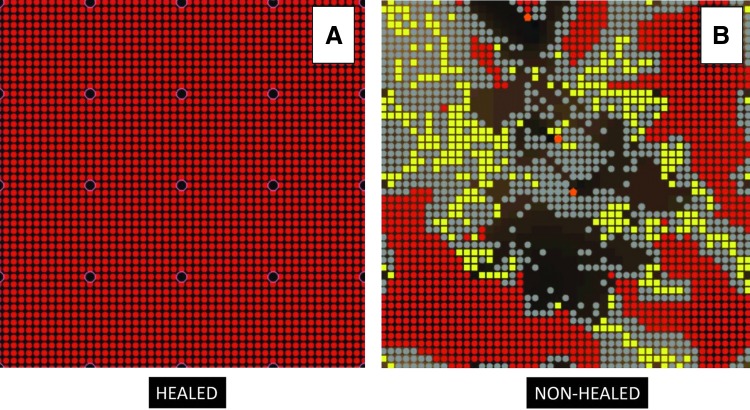
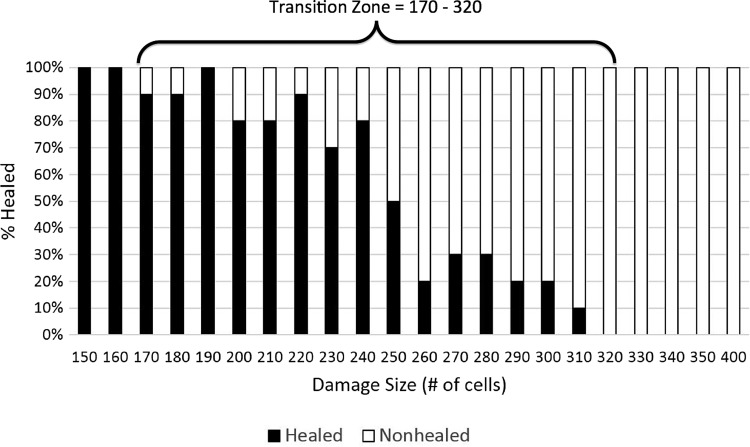
Approach: The Muscle Wound ABM (MWABM) incorporates muscle cells, neutrophils, macrophages, myoblasts, abstracted blood vessels, and avirulent/virulent bacteria to simulate the pathogenesis of SSIs. Simulated bacteria with virulence potential can mutate to possess resistance to reactive oxygen species and increased invasiveness. Simulated experiments (t=7 days) involved parameter sweeps of initial wound size to identify transition zones between healed and nonhealed wounds/SSIs, and to evaluate the effect of avirulent/virulent bacteria.
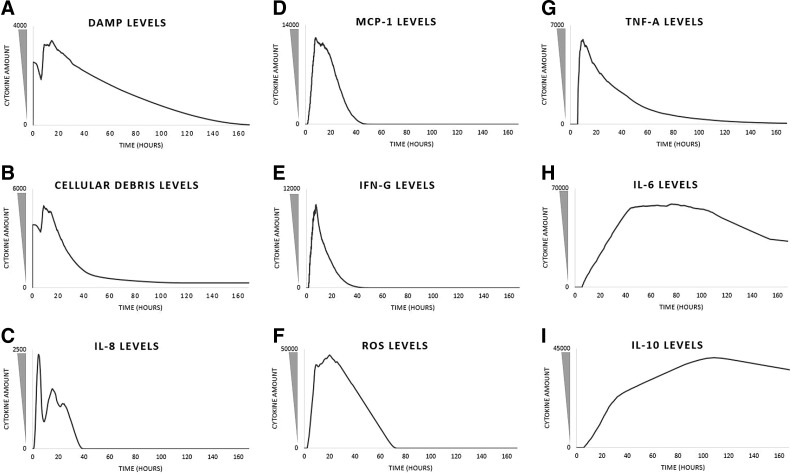
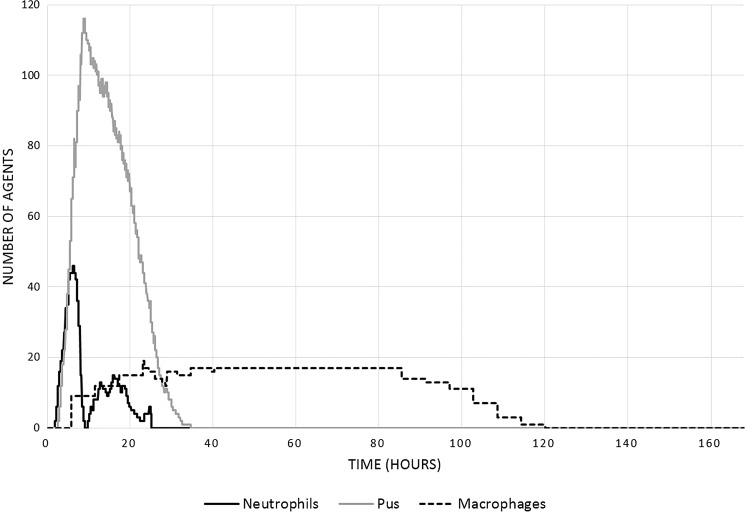
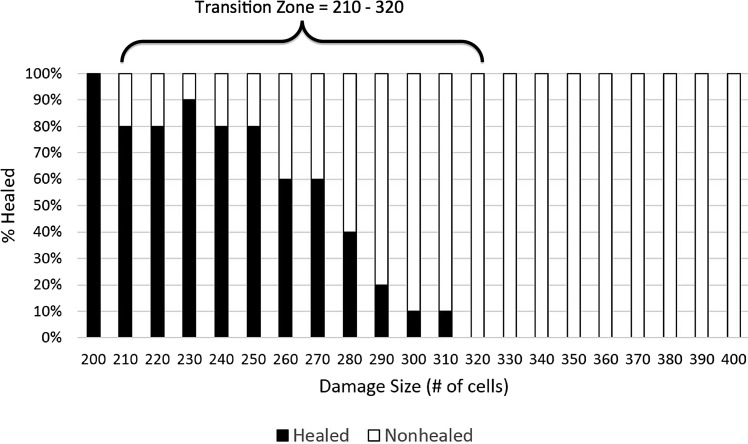
Results: The MWABM reproduced the dynamics of normal successful healing, including a transition zone in initial wound size beyond which healing was significantly impaired. Parameter sweeps with avirulent bacteria demonstrated that smaller wound sizes were associated with healing failure. This effect was even more pronounced with the addition of virulence potential to the contaminating bacteria.
Innovation: The MWABM integrates the myriad factors involved in the healing of a normal wound and the pathogenesis of SSIs. This type of model can serve as a useful framework into which more detailed mechanistic knowledge can be embedded.
Conclusion: Future work will involve more comprehensive representation of host factors, and especially the ability of those host factors to activate virulence potential in the microbes involved.
Figures

References
-
- Barie PS. Surgical site infections: epidemiology and prevention. Surg Infect (Larchmt) 2002;3(Suppl 1):S9. - PubMed
-
- Cruse P. Wound infection surveillance. Rev Infect Dis. 1981;3:734. - PubMed
-
- Anderson DJ. Surgical site infections. Infect Dis Clin North Am. 2011;25:135. - PubMed
-
- Owens CD. Stoessel K. Surgical site infections: epidemiology, microbiology and prevention. J Hosp Infect. 2008;70(Suppl 2):3. - PubMed
-
- Esposito S. Immune system and surgical site infection. J Chemother. 2011;S1:12. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
