

The Electrical Response to Injury: Molecular Mechanisms and Wound Healing
- PMID: 24761358
- PMCID: PMC3928722
- DOI: 10.1089/wound.2013.0442
The Electrical Response to Injury: Molecular Mechanisms and Wound Healing
Abstract
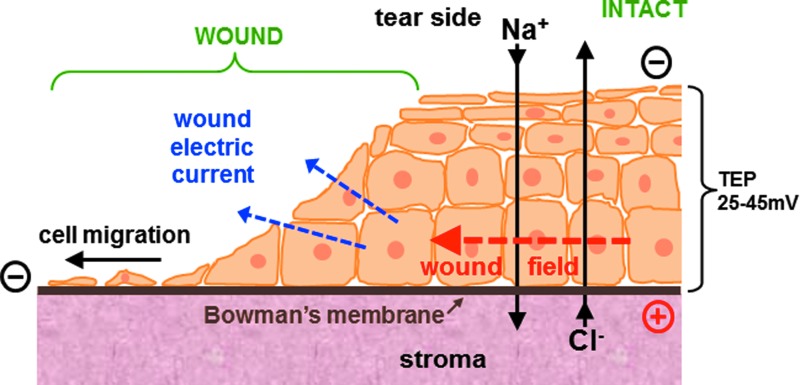
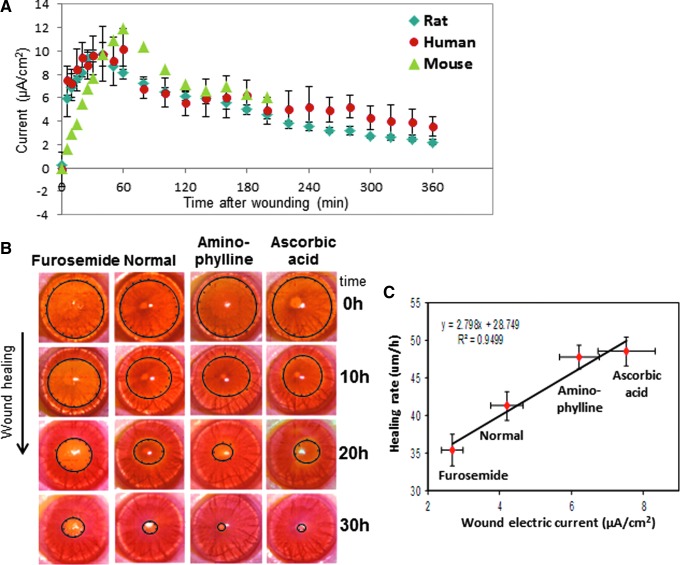
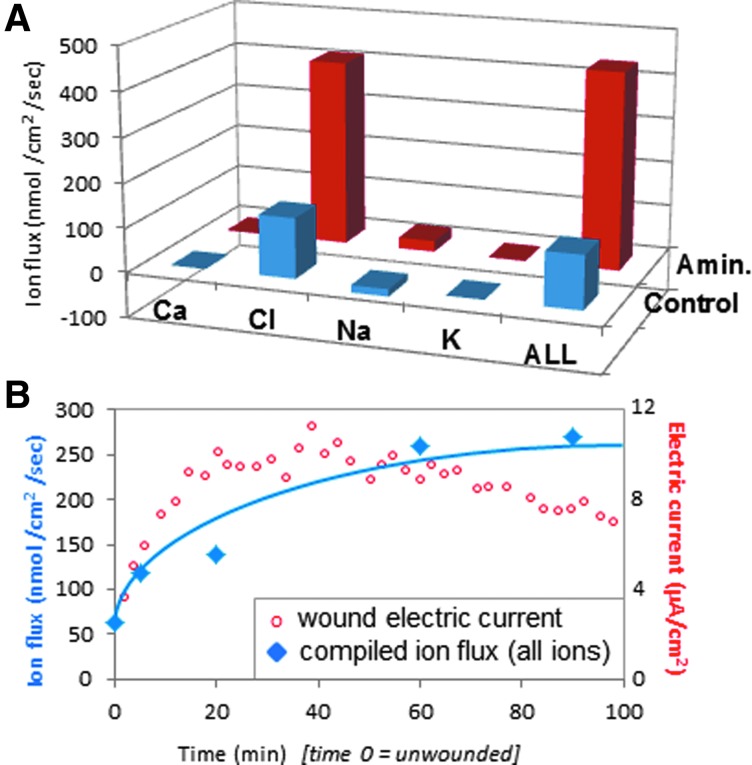
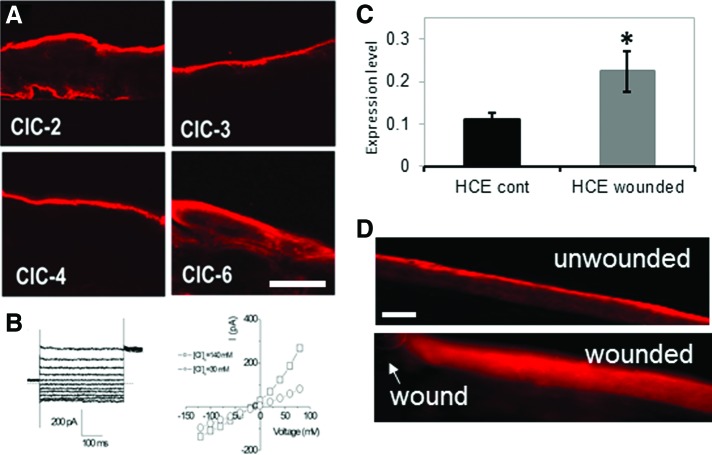
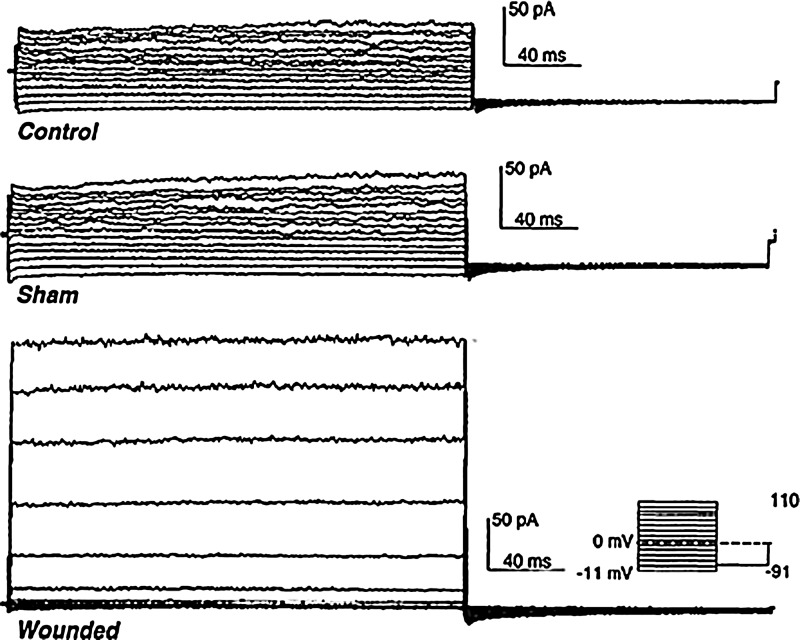
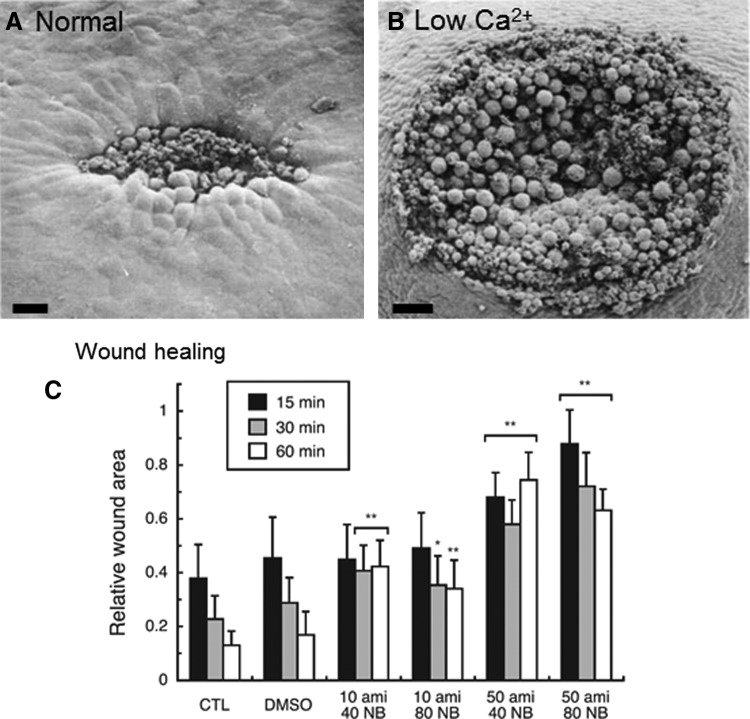
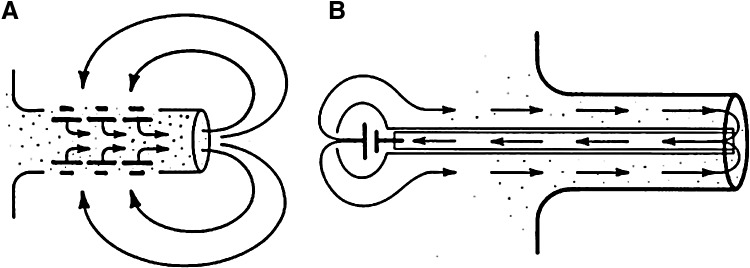
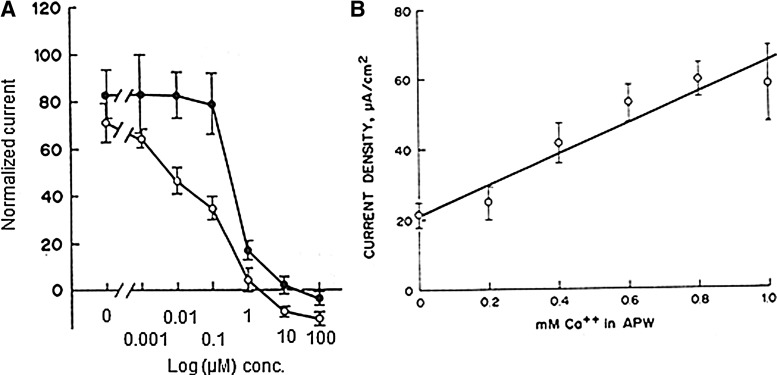
Significance: Natural, endogenous electric fields (EFs) and currents arise spontaneously after wounding of many tissues, especially epithelia, and are necessary for normal healing. This wound electrical activity is a long-lasting and regulated response. Enhancing or inhibiting this electrical activity increases or decreases wound healing, respectively. Cells that are responsible for wound closure such as corneal epithelial cells or skin keratinocytes migrate directionally in EFs of physiological magnitude. However, the mechanisms of how the wound electrical response is initiated and regulated remain unclear. Recent Advances: Wound EFs and currents appear to arise by ion channel up-regulation and redistribution, which are perhaps triggered by an intracellular calcium wave or cell depolarization. We discuss the possibility of stimulation of wound healing via pharmacological enhancement of the wound electric signal by stimulation of ion pumping. Critical Issues: Chronic wounds are a major problem in the elderly and diabetic patient. Any strategy to stimulate wound healing in these patients is desirable. Applying electrical stimulation directly is problematic, but pharmacological enhancement of the wound signal may be a promising strategy. Future Directions: Understanding the molecular regulation of wound electric signals may reveal some fundamental mechanisms in wound healing. Manipulating fluxes of ions and electric currents at wounds might offer new approaches to achieve better wound healing and to heal chronic wounds.
Figures

References
-
- Klyce SD: Transport of Na, Cl, and water by the rabbit corneal epithelium at resting potential. Am J Physiol 1975; 228:1446. - PubMed
-
- Foulds IS. and Barker AT: Human skin battery potentials and their possible role in wound healing. Br J Dermatol 1983; 109:515. - PubMed
-
- Barker AT, Jaffe LF, and Vanable JW, Jr: The glabrous epidermis of cavies contains a powerful battery. Am J Physiol 1982; 242:R358. - PubMed
-
- Mathias RT, Kistler J, and Donaldson P: The lens circulation. J Membr Biol 2007; 216:1. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
