

Efficacy of a multifactorial intervention on therapeutic adherence in patients with chronic obstructive pulmonary disease (COPD): a randomized controlled trial
- PMID: 24762026
- PMCID: PMC4011779
- DOI: 10.1186/1471-2466-14-70
Efficacy of a multifactorial intervention on therapeutic adherence in patients with chronic obstructive pulmonary disease (COPD): a randomized controlled trial
Abstract
Background: Therapeutic adherence of patients with chronic obstructive pulmonary disease (COPD) is poor. This study evaluated the effectiveness of a multifactorial intervention on improving the therapeutic adherence in chronic obstructive pulmonary disease (COPD) patients with scheduled inhalation therapy.
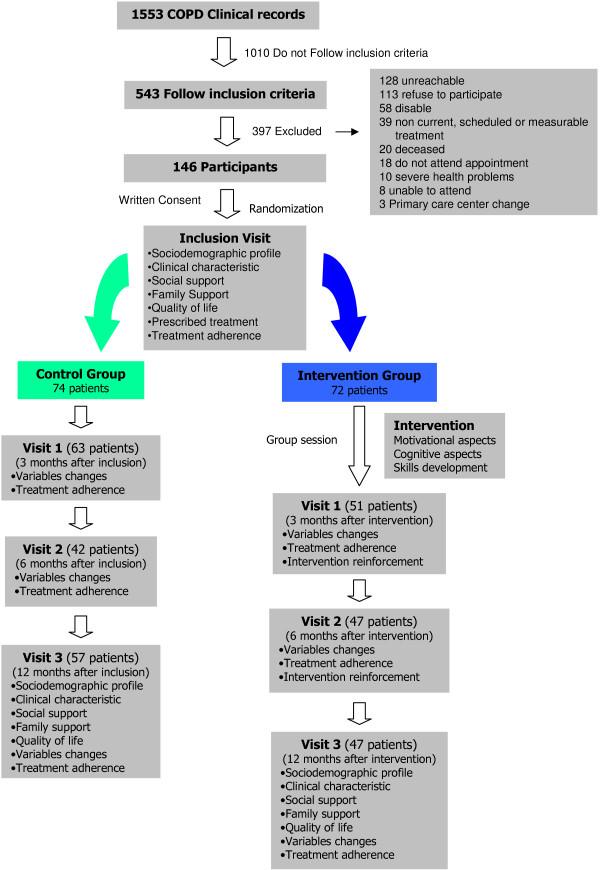
Methods: The study design consisted of a randomised controlled trial in a primary care setting. 146 patients diagnosed with COPD were randomly allocated into two groups using the block randomisation technique. One-year follow-ups with three visits were performed. The intervention consisted of motivational aspects related to adherence (beliefs and behaviour) in the form of group and individual interviews, cognitive aspects in the form of information about the illness and skills in the form of training in inhalation techniques. Cognitive-emotional aspects and training in inhalation techniques were reinforced during all visits of the intervention group. The main outcome measure was adherence to the medication regimen. Therapeutic adherence was determined by the percentage of patients classified as good adherent as evaluated by dose or pill count.
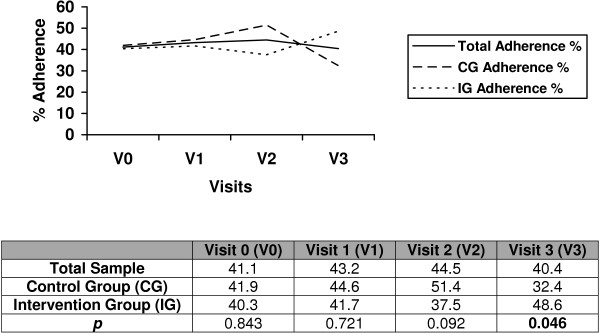
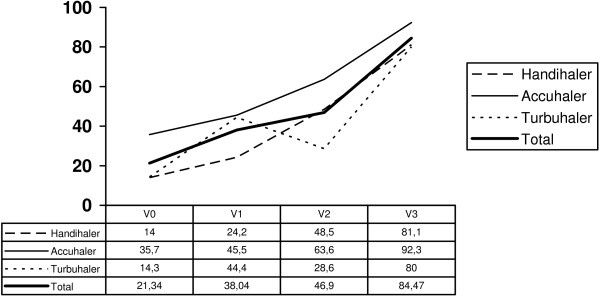
Results: Of the 146 participants (mean age 69.8 years, 91.8% males), 41.1% reported adherence (41.9% of the control group and 40.3% of the intervention group). When multifactorial intervention was applied, the reported adherence was 32.4% for the control group and 48.6% for the intervention group, which showed a statistically significant difference (p = 0.046). Number needed to treat is 6.37. In the intervention group, cognitive aspects increased by 23.7% and skilled performance of inhalation techniques increased by 66.4%. The factors related to adherence when multifactorial intervention was applied were the number of exacerbations (OR = 0.66), visits to health centre (OR = 0.93) and devices (OR = 2.4); illness severity (OR = 0.67), beta-2-adrenergic (OR = 0.16) and xantine (OR = 0.19) treatment; activity (OR = 1.03) and impact (OR = 1.03) scales of the Saint George Respiratory Questionnaire.
Conclusion: Application of the multifactorial intervention designed for this study (COPD information, dose reminders, audio-visual material, motivational aspects and training in inhalation techniques) resulted in an improvement in therapeutic adherence in COPD patients with scheduled inhalation therapy.
Trial registration: Current Controlled Trials ISRCTN18841601.
Figures
References
-
- Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, Mannino DM. On behalf of the BOLD Collaborative Research Group. International variation in the prevalence of COPD (The BOLD study): a population-based prevalence study. Lancet. 2007;370:741–750. doi: 10.1016/S0140-6736(07)61377-4. - DOI - PubMed
-
- Soriano JB, Miravitlles M, Borderías L, Duran-Tauleria E, Garcıía-Río F, Martínez J, Montemayor T, Muñoz L, Piñeiro L, Sánchez G, Serra J, Soler-Cataluña JJ, Torres A, Viejo JL, Sobradillo-Peña V, Ancochea J. Diferencias geográficas en la prevalencia de EPOC en España: relación con hábito tabáquico, tasas de mortalidad y otros determinantes. Arch Bronconeumol. 2010;46(10):522–530. doi: 10.1016/j.arbres.2010.06.008. - DOI - PubMed
-
- World Health Organization. World health statistics 2008. Available at: http://www.who.int/whosis/whostat/EN_WHS08_Full.pdf (accessed August 22, 2012)
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
