

Ventriculoarterial decoupling in human septic shock
- PMID: 24762124
- PMCID: PMC4056562
- DOI: 10.1186/cc13842
Ventriculoarterial decoupling in human septic shock
Abstract
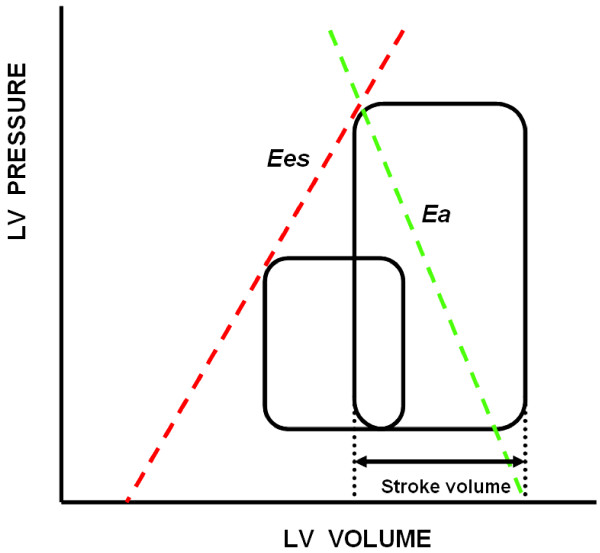
Introduction: Septic shock is the most severe manifestation of sepsis. It is characterized as a hypotensive cardiovascular state associated with multiorgan dysfunction and metabolic disturbances. Management of septic shock is targeted at preserving adequate organ perfusion pressure without precipitating pulmonary edema or massive volume overload. Cardiac dysfunction often occurs in septic shock patients and can significantly affect outcomes. One physiologic approach to detect the interaction between the heart and the circulation when both are affected is to examine ventriculoarterial coupling, which is defined by the ratio of arterial elastance (Ea) to left ventricular end-systolic elastance (Ees). In this study, we analyzed ventriculoarterial coupling in a cohort of patients admitted to ICUs who presented with vs without septic shock.
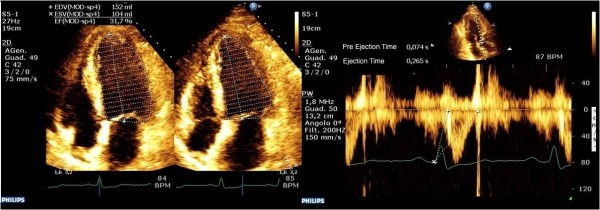
Methods: In this retrospective cross-sectional opportunity study, we measured routine hemodynamics using indwelling arterial and pulmonary arterial catheters and transthoracic echocardiograms in 25 septic patients (group S) and 25 non-septic shock patients (group C) upon ICU admission. Ees was measured by echocardiography using a single-beat (EesSB) method. Ea was calculated as 0.9 systolic arterial pressure/stroke volume, and then the Ea/EesSB ratio was calculated (normal value <1.36).
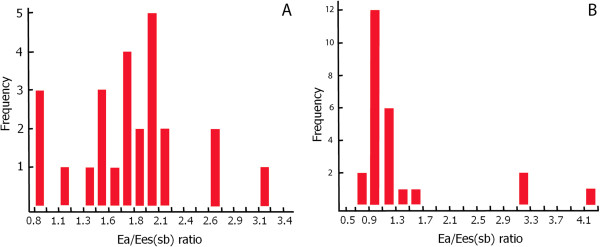
Results: In group S, 21 patients had an Ea/EesSB ratio >1.36 (uncoupled). The four patients with Ea/EesSB ratios ≤1.36 had higher EesSB values than patients with Ea/EesSB ratios >1.36 (P = 0.007), although Ea measurements were similar in both groups (P = 0.4). In group C, five patients had uncoupled Ea/EesSB ratios. No correlation was found between EesSB and left ventricular ejection fraction and between Ea/EesSB ratio and mixed venous oxygen saturation in septic shock patients.
Conclusions: Upon admission to the ICU, patients in septic shock often display significant ventriculoarterial decoupling that is associated with impaired left ventricular performance. Because Ea/Ees decoupling alters cardiovascular efficiency and cardiac energetic requirements independently of Ea or Ees, we speculate that septic patients with ventriculoarterial uncoupling may benefit from therapy aimed at normalizing the Ea/Ees ratio.
Figures
References
-
- Werdan K, Müller-Werdan U. Elucidating molecular mechanisms of septic cardiomyopathy—the cardiomyocyte model. Mol Cell Biochem. 1996;163–164:291–303. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
