

Expression of fibroblast growth factor 23, vitamin D receptor, and sclerostin in bone tissue from hypercalciuric stone formers
- PMID: 24763863
- PMCID: PMC4078962
- DOI: 10.2215/CJN.10030913
Expression of fibroblast growth factor 23, vitamin D receptor, and sclerostin in bone tissue from hypercalciuric stone formers
Abstract
Background and objectives: Increased bone resorption, low bone formation, and abnormal mineralization have been described in stone formers with idiopathic hypercalciuria. It has been previously shown that the receptor activator of NF-κB ligand mediates bone resorption in idiopathic hypercalciuria (IH). The present study aimed to determine the expression of fibroblast growth factor 23 (FGF-23), vitamin D receptor (VDR), and sclerostin in bone tissue from IH stone formers.
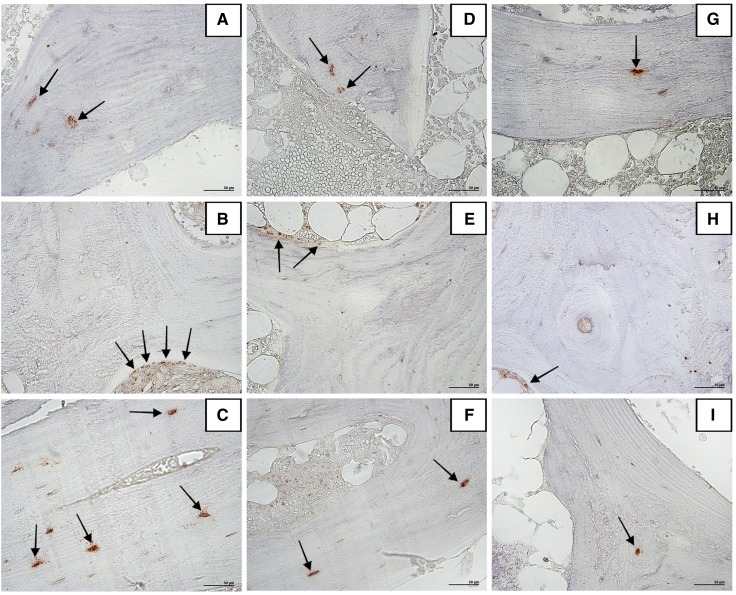
Design, setting, participants, & measurements: Immunohistochemical analysis was performed in undecalcified bone samples previously obtained for histomorphometry from 30 transiliac bone biopsies of idiopathic hypercalciuria stone-forming patients between 1992 and 2002 and 33 healthy individuals (controls). Serum parameters were obtained from their medical records.
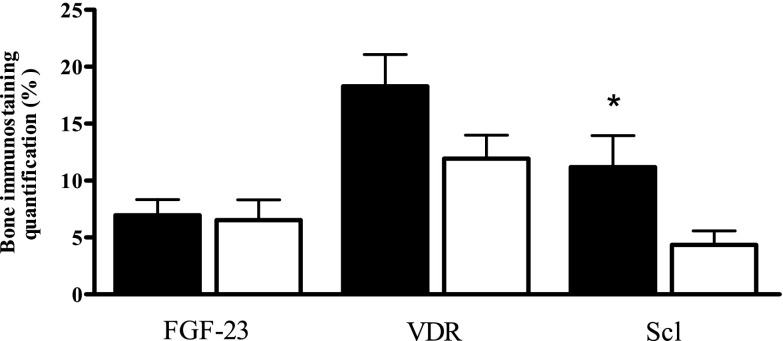
Results: Histomorphometry disclosed 21 IH patients with high and 9 IH patients with normal bone resorption. Importantly, eroded surfaces (ES/BS) from IH patients but not controls were significantly correlated with VDR immunostaining in osteoblasts (r=0.51; P=0.004), sclerostin immunostaining in osteocytes (r=0.41; P=0.02), and serum 1,25-dihydroxyvitamin D (r=0.55; P<0.01). Of note, both VDR and sclerostin immunostaining were significantly correlated with serum 1,25-dihydroxyvitamin D in IH patients (r=0.52; P=0.01 and r=0.53; P=0.02, respectively), although VDR and sclerostin expression did not differ between IH and controls. IH patients with high bone resorption exhibited a significantly stronger sclerostin immunostaining than IH patients with normal bone resorption. FGF-23 expression in osteocytes from IH patients did not differ from controls and was not correlated with any histomorphometric parameter.
Conclusions: These findings suggest the contribution of VDR and sclerostin, as well as 1,25-dihydroxyvitamin D, to increase bone resorption in idiopathic hypercalciuria but do not implicate FGF-23 in the bone alterations seen in these patients.
Keywords: FGF-23; VDR; hypercalciuria; immunohistochemistry; sclerostin.
Copyright © 2014 by the American Society of Nephrology.
Figures
Similar articles
-
RANKL is a mediator of bone resorption in idiopathic hypercalciuria.Clin J Am Soc Nephrol. 2008 Sep;3(5):1446-52. doi: 10.2215/CJN.00240108. Epub 2008 May 14. Clin J Am Soc Nephrol. 2008. PMID: 18480302 Free PMC article.
-
Vitamin D receptor in osteoblast lineage cells mediates increased sclerostin circulation and decreased bone formation in hypervitaminosis D.J Steroid Biochem Mol Biol. 2025 May;249:106711. doi: 10.1016/j.jsbmb.2025.106711. Epub 2025 Feb 20. J Steroid Biochem Mol Biol. 2025. PMID: 39986581
-
Elevated vitamin D receptor levels in genetic hypercalciuric stone-forming rats are associated with downregulation of Snail.J Bone Miner Res. 2010 Apr;25(4):830-40. doi: 10.1359/jbmr.091010. J Bone Miner Res. 2010. PMID: 19929616 Free PMC article.
-
Bone disease and idiopathic hypercalciuria.Semin Nephrol. 2008 Mar;28(2):133-42. doi: 10.1016/j.semnephrol.2008.01.006. Semin Nephrol. 2008. PMID: 18359394 Free PMC article. Review.
-
Osteocyte control of bone remodeling: is sclerostin a key molecular coordinator of the balanced bone resorption-formation cycles?Osteoporos Int. 2014 Dec;25(12):2685-700. doi: 10.1007/s00198-014-2808-0. Epub 2014 Jul 17. Osteoporos Int. 2014. PMID: 25030653 Review.
Cited by
-
Beta-thalassaemia major: Prevalence, risk factors and clinical consequences of hypercalciuria.Br J Haematol. 2022 Sep;198(5):903-911. doi: 10.1111/bjh.18345. Epub 2022 Jun 29. Br J Haematol. 2022. PMID: 35768889 Free PMC article.
-
Defining metabolic activity of nephrolithiasis - Appropriate evaluation and follow-up of stone formers.Asian J Urol. 2018 Oct;5(4):235-242. doi: 10.1016/j.ajur.2018.06.007. Epub 2018 Jun 26. Asian J Urol. 2018. PMID: 30364613 Free PMC article. Review.
-
Integrative microRNA-gene expression network analysis in genetic hypercalciuric stone-forming rat kidney.PeerJ. 2016 Mar 31;4:e1884. doi: 10.7717/peerj.1884. eCollection 2016. PeerJ. 2016. PMID: 27069814 Free PMC article.
-
Role of FGF23 in Pediatric Hypercalciuria.Biomed Res Int. 2017;2017:3781525. doi: 10.1155/2017/3781525. Epub 2017 Dec 31. Biomed Res Int. 2017. PMID: 29457024 Free PMC article. Clinical Trial.
-
Serum sclerostin is associated with recurrent kidney stone formation independent of hypercalciuria.Clin Kidney J. 2023 Nov 1;17(1):sfad256. doi: 10.1093/ckj/sfad256. eCollection 2024 Jan. Clin Kidney J. 2023. PMID: 38186870 Free PMC article.
References
-
- Heilberg IP, Martini LA, Szejnfeld VL, Carvalho AB, Draibe SA, Ajzen H, Ramos OL, Schor N: Bone disease in calcium stone forming patients. Clin Nephrol 42: 175–182, 1994 - PubMed
-
- Heilberg IP, Martini LA, Teixeira SH, Szejnfeld VL, Carvalho AB, Lobão R, Draibe SA: Effect of etidronate treatment on bone mass of male nephrolithiasis patients with idiopathic hypercalciuria and osteopenia. Nephron 79: 430–437, 1998 - PubMed
-
- Misael da Silva AM, dos Reis LM, Pereira RC, Futata E, Branco-Martins CT, Noronha IL, Wajchemberg BL, Jorgetti V: Bone involvement in idiopathic hypercalciuria. Clin Nephrol 57: 183–191, 2002 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
