

Impact of electrode design and surgical approach on scalar location and cochlear implant outcomes
- PMID: 24764083
- PMCID: PMC4209201
- DOI: 10.1002/lary.24728
Impact of electrode design and surgical approach on scalar location and cochlear implant outcomes
Abstract
Objectives/hypothesis: Three surgical approaches: cochleostomy (C), round window (RW), and extended round window (ERW); and two electrodes types: lateral wall (LW) and perimodiolar (PM), account for the vast majority of cochlear implantations. The goal of this study was to analyze the relationship between surgical approach and electrode type with final intracochlear position of the electrode array and subsequent hearing outcomes.
Study design: Comparative longitudinal study.
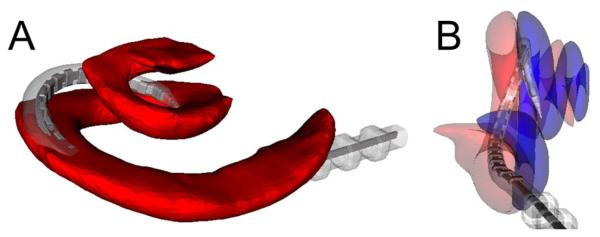
Methods: One hundred postlingually implanted adult patients were enrolled in the study. From the postoperative scan, intracochlear electrode location was determined and using rigid registration, transformed back to the preoperative computed tomography which had intracochlear anatomy (scala tympani and scala vestibuli) specified using a statistical shape model based on 10 microCT scans of human cadaveric cochleae. Likelihood ratio chi-square statistics were used to evaluate for differences in electrode placement with respect to surgical approach (C, RW, ERW) and type of electrode (LW, PM).
Results: Electrode placement completely within the scala tympani (ST) was more common for LW than were PM designs (89% vs. 58%; P < 0.001). RW and ERW approaches were associated with lower rates of electrode placement outside the ST than was the cochleostomy approach (9%, 16%, and 63%, respectively; P < 0.001). This pattern held true regardless of whether the implant was LW or PM. When examining electrode placement and hearing outcome, those with electrode residing completely within the ST had better consonant-nucleus-consonant word scores than did patients with any number of electrodes located outside the ST (P = 0.045).
Conclusion: These data suggest that RW and ERW approaches and LW electrodes are associated with an increased likelihood of successful ST placement. Furthermore, electrode position entirely within the ST confers superior audiological outcomes.
Level of evidence: 2b.
Keywords: Cochlear implant; cochleostomy; electrode; round window; sensorineural hearing loss.
© 2014 The American Laryngological, Rhinological and Otological Society, Inc.
Figures
References
-
- Friedland DR, Venick HS, Niparko JK. Choice of ear for cochlear implantation: the effect of history and residual hearing on predicted postoperative performance. Otol Neurotol. 2003;24:582–589. - PubMed
-
- Shipp DB, Nedzelski JM. Prognostic indicators of speech recognition performance in adult cochlear implant users: a prospective analysis. Ann Otolo Rhinol Laryngol Suppl. 1995;166:194–196. - PubMed
-
- Summerfield AQ, Marshall DH. Preoperative predictors of outcomes from cochlear implantation in adults: performance and quality of life. Ann Otolo Rhinol Laryngol Suppl. 1995;166:105–108. - PubMed
-
- Blamey P, Arndt P, Bergeron F, et al. Factors affecting auditory performance of postlinguistically deaf adults using cochlear implants. Audiol Neurotol. 1996;1:293–306. - PubMed
-
- Rubinstein JT, Parkinson WS, Tyler RS, Gantz BJ. Residual speech recognition and cochlear implant performance: effects of implantation criteria. Am J Otol. 1999;20:445–452. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
