

Effect of resistance training on non-alcoholic fatty-liver disease a randomized-clinical trial
- PMID: 24764677
- PMCID: PMC3989975
- DOI: 10.3748/wjg.v20.i15.4382
Effect of resistance training on non-alcoholic fatty-liver disease a randomized-clinical trial
Abstract
Aim: To evaluate the effect of resistance training (RT) on non alcoholic liver disease (NAFLD) patients.
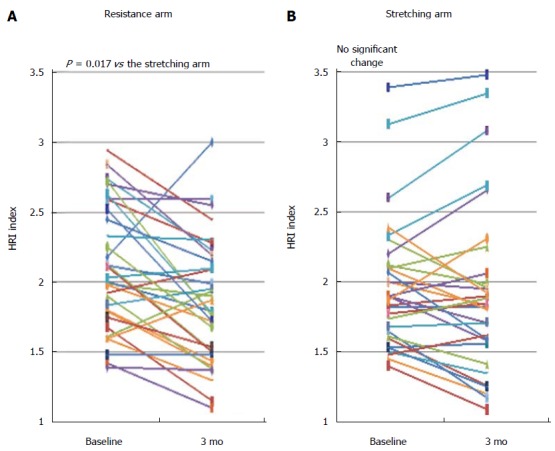
Methods: A randomized clinical trial enrolling NAFLD patients without secondary liver disease (e.g., without hepatitis B virus, hepatitis C virus or excessive alcohol consumption). Patients were randomly allocated either to RT, three times weekly, for 3 mo or a control arm consisting of home stretching. The RT included leg press, chest press, seated rowing, latissimus pull down etc. with 8-12 repetitions, 3 sets for each exercise, for a total duration of 40 min. Hepatic ultrasound, fasting blood tests, anthropometrics and body composition by dual energy X-ray absorptiometry were assessed. At baseline and follow-up, patients filled out a detailed semi-quantitative food frequency questionnaire reporting their habitual nutritional intake. Steatosis was quantified by the hepatorenal-ultrasound index (HRI) representing the ratio between the brightness level of the liver and the right kidney. The HRI has been previously demonstrated to be highly reproducible and was validated against liver biopsy and proton magnetic resonance spectroscopy.
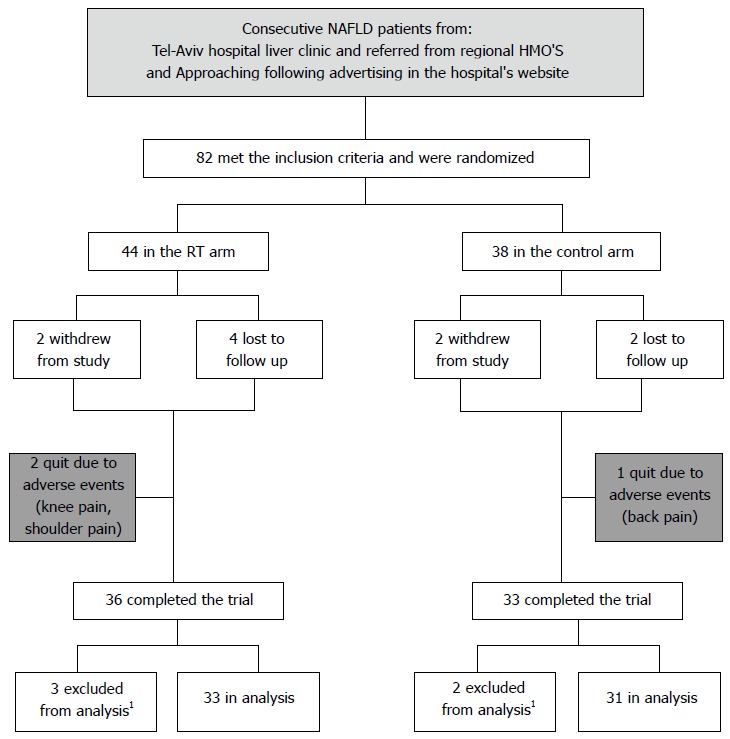
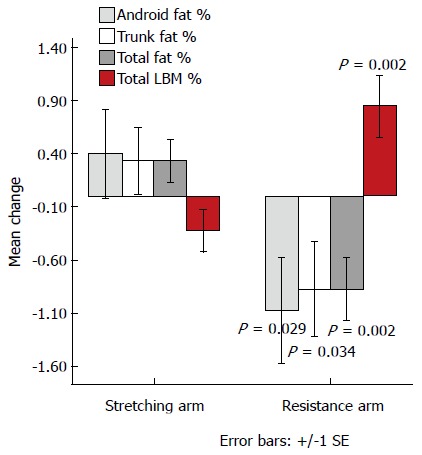
Results: Eighty two patients with primary NAFLD were randomized to receive 3 mo of either RT or stretching. After dropout or exclusion from analysis because of protocol violation (weight change > 3 kg), thirty three patients in the RT arm and 31 in the stretching arm completed the study per protocol. All baseline characteristics were similar for the two treatment groups with respect to demographics, anthropometrics and body composition, blood tests and liver steatosis on imaging. HRI score was reduced significantly in the RT arm as compared to the stretching arm (-0.25 ± 0.37 vs -0.05 ± 0.28, P = 0.017). The RT arm had a significantly higher reduction in total, trunk and android fat with increase in lean body mass. There was no correlation between the reduction in HRI in the RT arm and weight change during the study, but it was positively correlated with the change in trunk fat (r = 0.37, P = 0.048). The RT arm had a significant reduction in serum ferritin and total cholesterol. There was no significant difference between arms in dietary changes and these did not correlate with HRI change.
Conclusion: Three months RT improves hepatic fat content accompanied by favorable changes in body composition and ferritin. RT may serve as a complement to treatment of NAFLD.
Keywords: Abdominal fat; Nutrition; Obesity; Physical activity; Resistance exercise.
Figures
References
-
- Duncan GE, Perri MG, Theriaque DW, Hutson AD, Eckel RH, Stacpoole PW. Exercise training, without weight loss, increases insulin sensitivity and postheparin plasma lipase activity in previously sedentary adults. Diabetes Care. 2003;26:557–562. - PubMed
-
- Bellentani S, Dalle Grave R, Suppini A, Marchesini G. Behavior therapy for nonalcoholic fatty liver disease: The need for a multidisciplinary approach. Hepatology. 2008;47:746–754. - PubMed
-
- Kraemer WJ, Ratamess NA. Fundamentals of resistance training: progression and exercise prescription. Med Sci Sports Exerc. 2004;36:674–688. - PubMed
-
- Pollock ML, Franklin BA, Balady GJ, Chaitman BL, Fleg JL, Fletcher B, Limacher M, Piña IL, Stein RA, Williams M, et al. AHA Science Advisory. Resistance exercise in individuals with and without cardiovascular disease: benefits, rationale, safety, and prescription: An advisory from the Committee on Exercise, Rehabilitation, and Prevention, Council on Clinical Cardiology, American Heart Association; Position paper endorsed by the American College of Sports Medicine. Circulation. 2000;101:828–833. - PubMed
-
- Zelber-Sagi S, Nitzan-Kaluski D, Goldsmith R, Webb M, Zvibel I, Goldiner I, Blendis L, Halpern Z, Oren R. Role of leisure-time physical activity in nonalcoholic fatty liver disease: a population-based study. Hepatology. 2008;48:1791–1798. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
