

CD30+ extranodal natural killer/T-cell lymphoma mimicking phlegmonous myositis: A case report
- PMID: 24765148
- PMCID: PMC3997696
- DOI: 10.3892/ol.2014.1924
CD30+ extranodal natural killer/T-cell lymphoma mimicking phlegmonous myositis: A case report
Abstract
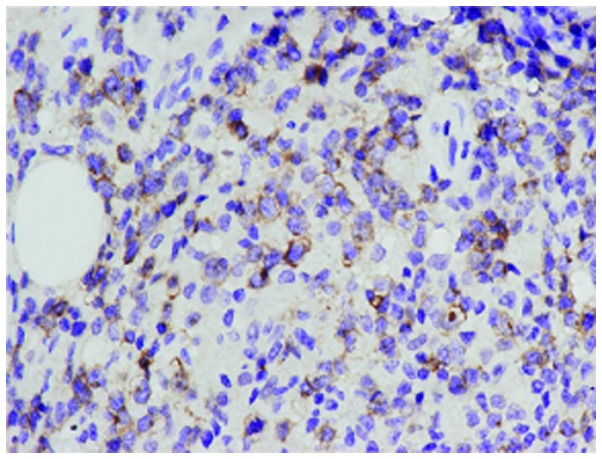
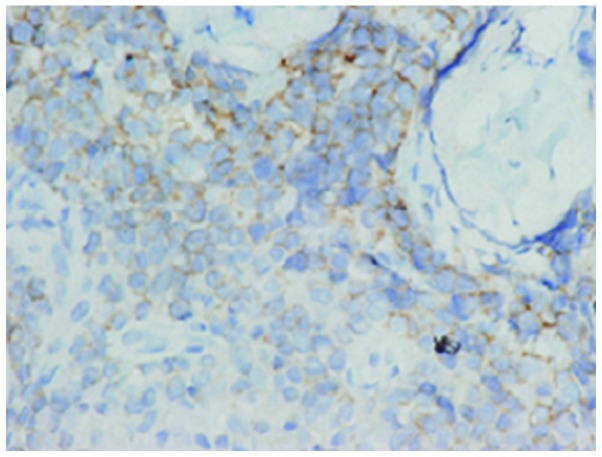
The current study presents a case of a 23-year-old male with CD30+ nasal-type extranodal natural killer/T-cell lymphoma (NKTL), with unusual clinical features mimicking phlegmonous myositis. The patient initially presented with swelling and tenderness of the left lower limb, particularly around the left ankle. One month later, pharyngalgia and fever developed and the patient was treated with antibiotics for the phlegmonous inflammation, however, the symptoms were not relieved. A muscle biopsy was performed on the lesion and revealed diffuse infiltration of atypical lymphoid cells with irregular nuclei. Immunohistochemistry showed staining for CD3ɛ(-), CD20(-), CD45(+), CD30(+) and CD56(+) presented with positive staining for certain tumor cells, granzyme B(+), activin receptor-like kinase 1(-), Ki-67(+) and Epstein-Barr virus-encoded small RNA(+), which indicated nasal-type extranodal NKTL. The present case emphasized that extranodal NKTL may be a rare cause of phlegmonous inflammation and fever of undetermined origin.
Keywords: extranodal natural killer/T-cell lymphoma; fever of undetermined origin; nasal-type; phlegmonous myositis.
Figures

Similar articles
-
Penile metastasis secondary to nasal-type extranodal natural killer/T-cell lymphoma: A case report and review of the literature.Oncol Lett. 2018 May;15(5):8034-8038. doi: 10.3892/ol.2018.8288. Epub 2018 Mar 16. Oncol Lett. 2018. PMID: 29725484 Free PMC article.
-
A case of CD30+ nasal natural killer/T-cell lymphoma.Am J Dermatopathol. 2008 Dec;30(6):567-71. doi: 10.1097/DAD.0b013e318184bc3f. Am J Dermatopathol. 2008. PMID: 19033930
-
A case of Epstein-Barr virus-associated natural killer/T-cell lymphoma presenting as dermatomyositis: extranodal relapse after 7 years in remission.Mod Rheumatol. 2005;15(6):435-9. doi: 10.1007/s10165-005-0432-8. Mod Rheumatol. 2005. PMID: 17029109
-
Clinicopathological study of pulmonary extranodal nature killer/T-cell lymphoma, nasal type and literature review.Pathol Res Pract. 2015 Jul;211(7):544-9. doi: 10.1016/j.prp.2015.04.002. Epub 2015 Apr 17. Pathol Res Pract. 2015. PMID: 25953340 Review.
-
Primary spleen extranodal NK/T cell lymphoma, nasal type, with bone marrow involvement and CD30 positive expression: a case report and literature review.Diagn Pathol. 2014 Sep 3;9:169. doi: 10.1186/s13000-014-0169-9. Diagn Pathol. 2014. PMID: 25183396 Free PMC article. Review.
Cited by
-
Extranodal natural killer/T cell lymphoma of the skeletal muscle.Skeletal Radiol. 2025 Jan;54(1):141-146. doi: 10.1007/s00256-024-04680-w. Epub 2024 Apr 20. Skeletal Radiol. 2025. PMID: 38642301 Free PMC article.
-
Muscular involvement of extranodal natural killer/T cell lymphoma misdiagnosed as polymyositis: A case report and review of literature.World J Clin Cases. 2020 Mar 6;8(5):963-970. doi: 10.12998/wjcc.v8.i5.963. World J Clin Cases. 2020. PMID: 32190634 Free PMC article.
References
-
- Chen CS, Miller NR, Lane A, Eberhart C. Third cranial nerve palsy caused by intracranial extension of a sino-orbital natural killer T-cell lymphoma. J Neuroophthalmol. 2008;28:31–35. - PubMed
-
- Yousuf SJ, Kumar N, Kidwell ED, Jr, Copeland RA., Jr Rapidly fatal nasal natural killer/T-cell lymphoma: orbital and ocular adnexal presentations. Orbit. 2011;30:120–121. - PubMed
-
- Stokkermans-Dubois J, Jouary T, Vergier B, Delaunay MM, Taieb A. A case of primary cutaneous nasal type NK/T-cell lymphoma and review of the literature. Dermatology. 2006;213:345–349. - PubMed
-
- Min HS, Hyun CL, Paik JH, Jeon YK, Choi G, Park SH, et al. An autopsy case of aggressive CD30+ extra-nodal NK/T-cell lymphoma initially manifested with granulomatous myositis. Leuk Lymphoma. 2006;47:347–352. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous