

Sacral chordoma in an adult showing an aggressive clinical course: A case report
- PMID: 24765153
- PMCID: PMC3997712
- DOI: 10.3892/ol.2014.1892
Sacral chordoma in an adult showing an aggressive clinical course: A case report
Abstract
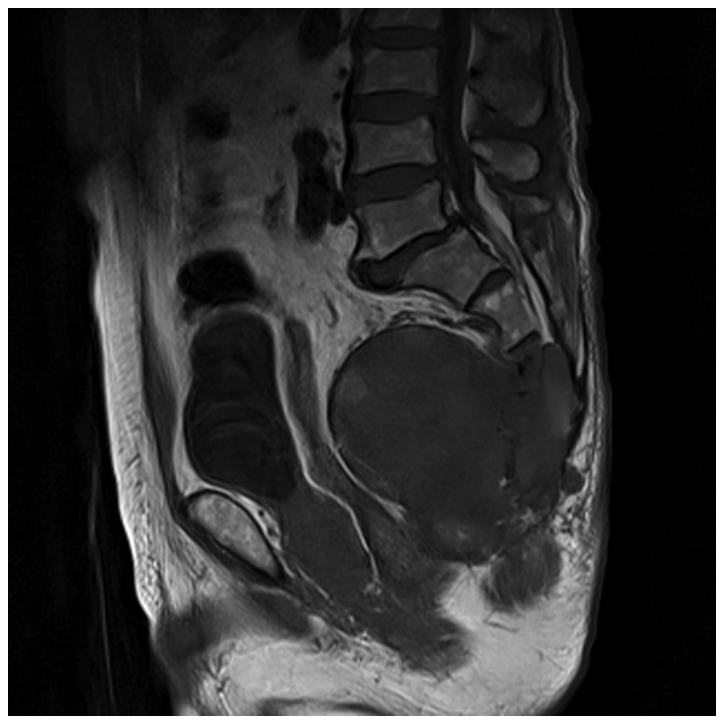
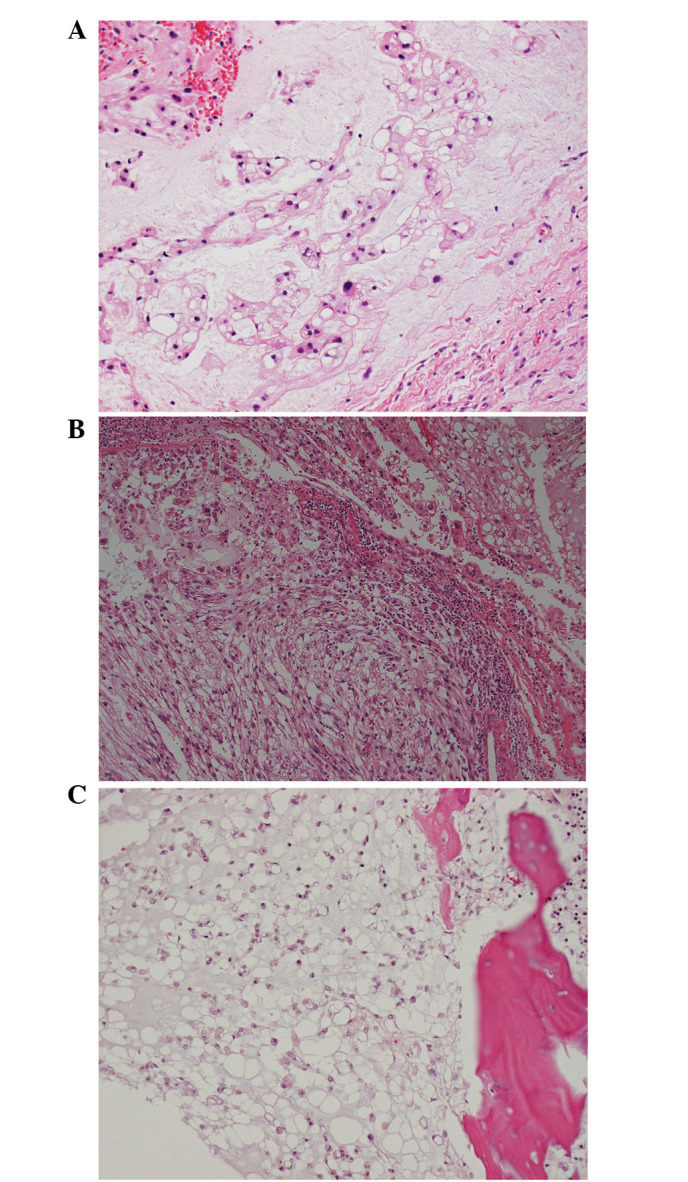
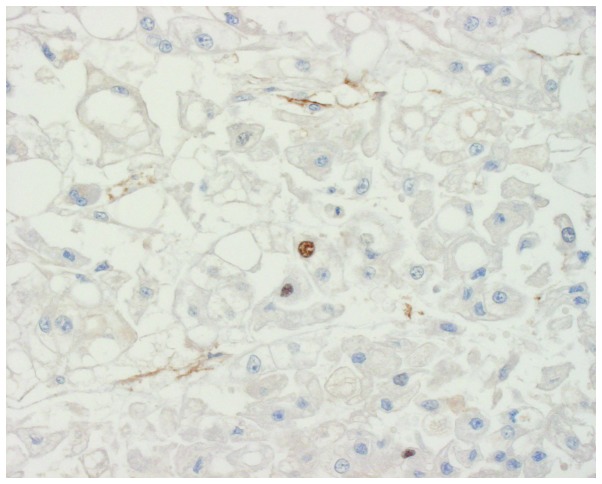
The current report presents a case of a 78-year-old male with sacral chordoma, showing an aggressive clinical course. The patient underwent sacral resection, however, nine months later, multiple metastases were detected by magnetic resonance imaging. The metastases progressed rapidly and 15 months following surgery the patient succumbed to respiratory dysfunction. An autopsy revealed multiple metastases of the lung, liver, heart, kidneys and vertebrae. Pathologically, the tumors did not show proliferation of anaplastic cells or dedifferentiation; however, the metastatic tumor cells were smaller than the primary tumor cells. The Ki-67 labeling indices were <5% in all of the patient's tumors, therefore, the capacity for cellular proliferation of the tumors was considered to be low. Chordoma in adults are generally slow-growing tumors and are associated with a relatively prolonged course and frequent local recurrences. Therefore, it must be recognized that chordoma may grow rapidly and show an aggressive clinical course, even when the Ki-67 labeling index is low.
Keywords: Ki-67; aggressive; chordoma; sacrum.
Figures

Similar articles
-
Natural History of a Patient with Sacral Chordoma: Case Report and Literature Review.World Neurosurg. 2020 Jul;139:132-135. doi: 10.1016/j.wneu.2020.03.214. Epub 2020 Apr 13. World Neurosurg. 2020. PMID: 32298828 Review.
-
Sacral chordoma: a clinical review of 101 cases with 30-year experience in a single institution.Spine J. 2019 May;19(5):869-879. doi: 10.1016/j.spinee.2018.11.002. Epub 2018 Nov 14. Spine J. 2019. PMID: 30445184
-
[Sacral chordoma: retrospective review of 11 surgically treated cases].Rev Chir Orthop Reparatrice Appar Mot. 2000 Nov;86(7):684-93. Rev Chir Orthop Reparatrice Appar Mot. 2000. PMID: 11104990 French.
-
Rare case of neglected large sacral Chordoma in a young female treated by wide En bloc resection and Sacrectomy.BMC Cancer. 2018 Nov 14;18(1):1112. doi: 10.1186/s12885-018-5012-3. BMC Cancer. 2018. PMID: 30428857 Free PMC article.
-
Review of current treatment of sacral chordoma.Orthop Surg. 2009 Aug;1(3):238-44. doi: 10.1111/j.1757-7861.2009.00027.x. Orthop Surg. 2009. PMID: 22009849 Free PMC article. Review.
Cited by
-
Prognostic significance of pretreatment plasma D-dimer levels in patients with spinal chordoma: a retrospective cohort study.Eur Spine J. 2019 Jun;28(6):1480-1490. doi: 10.1007/s00586-018-05872-4. Epub 2019 Jan 25. Eur Spine J. 2019. PMID: 30684054
-
Genomic and transcriptomic characterization of skull base chordoma.Oncotarget. 2017 Jan 3;8(1):1321-1328. doi: 10.18632/oncotarget.13616. Oncotarget. 2017. PMID: 27901492 Free PMC article.
References
-
- Huvos AG, editor. Bone Tumors: Diagnosis, Treatment and Prognosis. WB Saunders; Philadelphia, PA: 1979. pp. 373–391.
-
- Unni KK, editor. Dahlin’s Bone Tumors: General Aspects and Data on 11,087 cases. 5th edition. Lippincott-Raven; Philadelphia, PA: 1996. pp. 291–305.
-
- Chambers PW, Schwinn CP. Chordoma: A clinicopathologic study of metastasis. Am J Clin Pathol. 1979;72:765–776. - PubMed
-
- Hruban RH, May M, Marcove RC, Huvos AG. Lumbo-sacral chordoma with high-grade malignant cartilaginous and spindle cell components. Am J Surg Pathol. 1990;14:384–389. - PubMed
-
- Coffin CM, Swanson PE, Wick MR, Dehner LP. Chordoma in childhood and adolescence: A clinicopathologic analysis of 12 cases. Arch Pathol Lab Med. 1993;117:927–933. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources