

The dilemma of treating vertebrobasilar dolichoectasia
- PMID: 24765483
- PMCID: PMC3981198
- DOI: 10.4081/cp.2012.e84
The dilemma of treating vertebrobasilar dolichoectasia
Abstract
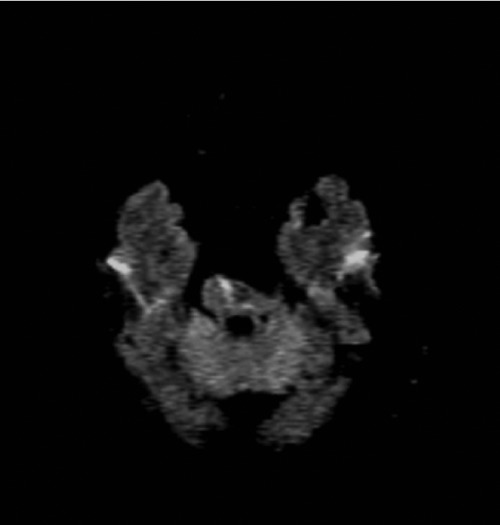
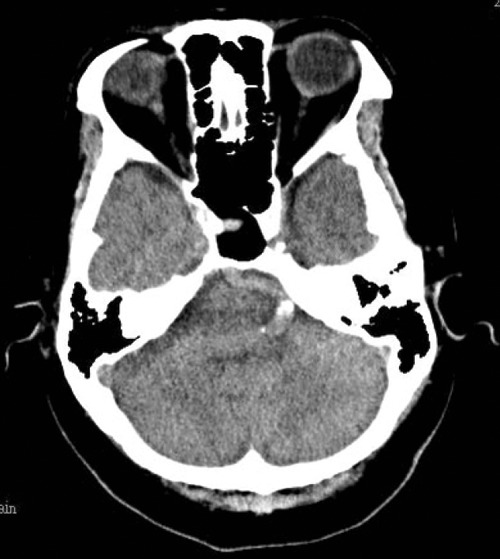
Vertebrobasilar dolichoectasia (VBD) is a common phenomenon among people over 50 years old, and the related clinical expressions are varied. One of our VBD patients presented with brainstem infarction initially, received low molecular weight heparin treatment, and developed rupture of the dolichoectasia segment. Another patient with a similar-sized VBD experienced recurrent brainstem infarction three times over 2 years, despite higher bleeding tendency and long-term antiplatelet treatment. The third patient with a smallersized VBD, had left hemiplegia and received intravenous recombinant tissue plasminogen activator within 3 h, totally recovered with no lesions detected on brain Magnetic Resonance Imaging (MRI). The pathophysiology of VBD is unique, its prevalence and risks of ischemic stroke and intracranial hemorrhage both increase as the degree of arterial dolichoectasia extends, making the strategy of management quite a challenge. The best management of VBD is controlling arterial hypertension and following up with image studies regularly to detect the early extension of VBD degree.
Keywords: basilar artery occlusion; ischemic stroke; non-saccular intracranial aneurysm; subarachnoid hemorrhage.; vertebrobasilar dolichoectasia.
Figures








Similar articles
-
Hemifacial spasm and recurrent stroke due to vertebrobasilar dolichoectasia coexisting with saccular aneurysm of the basilar artery: a case report.Turk Neurosurg. 2013;23(2):282-4. doi: 10.5137/1019-5149.JTN.4889-11.1. Turk Neurosurg. 2013. PMID: 23546920
-
Imaging features of vertebrobasilar dolichoectasia combined with posterior circulation ischemic stroke: A vessel wall magnetic resonance imaging study.Eur J Radiol. 2023 Sep;166:110971. doi: 10.1016/j.ejrad.2023.110971. Epub 2023 Jul 11. Eur J Radiol. 2023. PMID: 37506476
-
Studying the imaging features and infarction mechanism of vertebrobasilar dolichoectasia with high-resolution magnetic resonance imaging.Brain Pathol. 2023 Mar;33(2):e13135. doi: 10.1111/bpa.13135. Epub 2023 Jan 31. Brain Pathol. 2023. PMID: 36718993 Free PMC article.
-
Two types of arteriopathies, arteriomegaly and aneurysms, frequently develop at diverse locations in vertebrobasilar dolichoectasia patients: A retrospective analysis and a meta-analysis.J Clin Neurosci. 2025 Mar;133:111027. doi: 10.1016/j.jocn.2024.111027. Epub 2025 Jan 3. J Clin Neurosci. 2025. PMID: 39755032
-
Multimodality Imaging of Vertebrobasilar Dolichoectasia: Clinical Presentations and Imaging Spectrum.Radiographics. 2016 Jul-Aug;36(4):1129-46. doi: 10.1148/rg.2016150032. Epub 2016 Jun 17. Radiographics. 2016. PMID: 27315445 Review.
Cited by
-
Intracranial Arterial Dolichoectasia.Front Neurol. 2017 Jul 17;8:344. doi: 10.3389/fneur.2017.00344. eCollection 2017. Front Neurol. 2017. PMID: 28769872 Free PMC article. Review.
-
Vascular Anomaly Presenting as Neurological Crisis: A Case Report of Dolichoectasia-Induced Seizures.Cureus. 2024 Sep 2;16(9):e68443. doi: 10.7759/cureus.68443. eCollection 2024 Sep. Cureus. 2024. PMID: 39360073 Free PMC article.
-
Outcomes in Symptomatic Patients With Vertebrobasilar Dolichoectasia Following Endovascular Treatment.Front Neurol. 2019 Jun 13;10:610. doi: 10.3389/fneur.2019.00610. eCollection 2019. Front Neurol. 2019. PMID: 31263445 Free PMC article.
-
Chronic cerebral hypoperfusion and plasticity of the posterior cerebral artery following permanent bilateral common carotid artery occlusion.Korean J Physiol Pharmacol. 2017 Nov;21(6):643-650. doi: 10.4196/kjpp.2017.21.6.643. Epub 2017 Oct 30. Korean J Physiol Pharmacol. 2017. PMID: 29200907 Free PMC article.
-
Ischemic stroke with extensive vasculopathy in a patient with neurofibromatosis type 1.Radiol Case Rep. 2022 Jul 16;17(9):3370-3372. doi: 10.1016/j.radcr.2022.05.029. eCollection 2022 Sep. Radiol Case Rep. 2022. PMID: 35865363 Free PMC article.
References
-
- Flemming KD, Wiebers DO, Brown RD, Jr, et al. The natural history of radiographically defined vertebrobasilar nonsaccular intracranial aneurysms. Cerebrovasc Dis. 2005;20:270–9. - PubMed
-
- Flemming KD, Wiebers DO, Brown RD, Jr, et al. Prospective risk of hemorrhage in patients with vertebrobasilar nonsaccular intracranial aneurysm. J Neurosurg. 2004;101:82–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
