

Thromboprophylaxis patterns and determinants in critically ill patients: a multicenter audit
- PMID: 24766968
- PMCID: PMC4057024
- DOI: 10.1186/cc13844
Thromboprophylaxis patterns and determinants in critically ill patients: a multicenter audit
Abstract
Introduction: Heparin is safe and prevents venous thromboembolism in critical illness. We aimed to determine the guideline concordance for thromboprophylaxis in critically ill patients and its predictors, and to analyze factors associated with the use of low molecular weight heparin (LMWH), as it may be associated with a lower risk of pulmonary embolism and heparin-induced thrombocytopenia without increasing the bleeding risk.
Methods: We performed a retrospective audit in 28 North American intensive care units (ICUs), including all consecutive medical-surgical patients admitted in November 2011. We documented ICU thromboprophylaxis and reasons for omission. Guideline concordance was determined by adding days in which patients without contraindications received thromboprophylaxis to days in which patients with contraindications did not receive it, divided by the total number of patient-days. We used multilevel logistic regression including time-varying, center and patient-level covariates to determine the predictors of guideline concordance and use of LMWH.
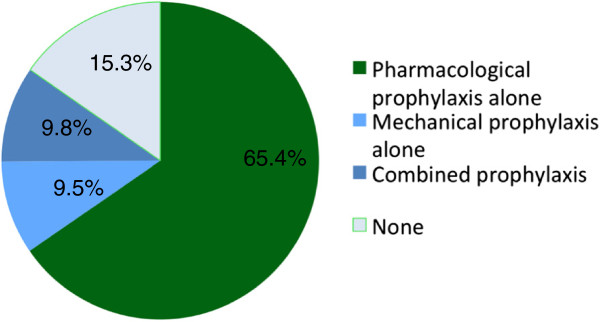
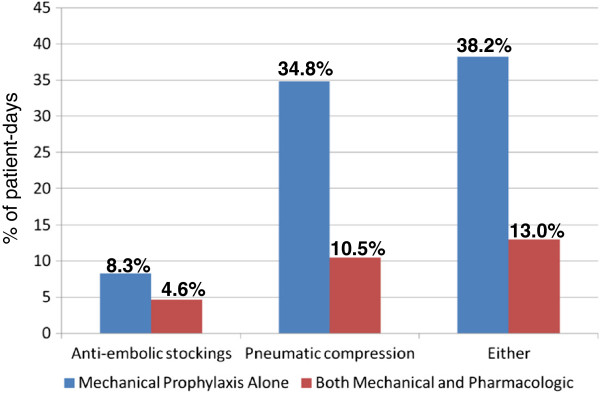
Results: We enrolled 1,935 patients (62.3 ± 16.7 years, Acute Physiology and Chronic Health Evaluation [APACHE] II score 19.1 ± 8.3). Patients received thromboprophylaxis with unfractionated heparin (UFH) (54.0%) or LMWH (27.6%). Guideline concordance occurred for 95.5% patient-days and was more likely in patients who were sicker (odds ratio (OR) 1.49, 95% confidence interval (CI) 1.17, 1.75 per 10-point increase in APACHE II), heavier (OR 1.32, 95% CI 1.05, 1.65 per 10-m/kg2 increase in body mass index), had cancer (OR 3.22, 95% CI 1.81, 5.72), previous venous thromboembolism (OR 3.94, 95% CI 1.46,10.66), and received mechanical ventilation (OR 1.83, 95% CI 1.32,2.52). Reasons for not receiving thromboprophylaxis were high risk of bleeding (44.5%), current bleeding (16.3%), no reason (12.9%), recent or upcoming invasive procedure (10.2%), nighttime admission or discharge (9.7%), and life-support limitation (6.9%). LMWH was less often administered to sicker patients (OR 0.65, 95% CI 0.48, 0.89 per 10-point increase in APACHE II), surgical patients (OR 0.41, 95% CI 0.24, 0.72), those receiving vasoactive drugs (OR 0.47, 95% CI 0.35, 0.64) or renal replacement therapy (OR 0.10, 95% CI 0.05, 0.23).
Conclusions: Guideline concordance for thromboprophylaxis was high, but LMWH was less commonly used, especially in patients who were sicker, had surgery, or received vasopressors or renal replacement therapy, representing a potential quality improvement target.
Figures
References
-
- Kahn SR, Lim W, Dunn AS, Cushman M, Dentali F, Akl EA, Cook DJ, Balekian AA, Klein RC, Le H, Schulman S, Murad MH. Prevention of VTE in nonsurgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141:e195S–e226S. - PMC - PubMed
-
- Prevention of Venous Thromboembolism after Injury. Evidence Report/Technology Assessment: Number 22. [ http://archive.ahrq.gov/clinic/epcsums/vtsumm.htm] - PMC - PubMed
-
- Venous Thromboembolism. [ http://www.jointcommission.org/venous_thromboembolism/]
-
- Required Organizational Practices 2012. [ http://www.accreditation.ca/sites/default/files/rop-handbook-2014-en.pdf]
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
