

Drivers of hospitalization for patients with atrial fibrillation: Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF)
- PMID: 24766985
- PMCID: PMC4006943
- DOI: 10.1016/j.ahj.2014.02.003
Drivers of hospitalization for patients with atrial fibrillation: Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF)
Abstract
Background: Atrial fibrillation (AF) is the most common cardiac dysrhythmia and contributes significantly to health care expenditures. We sought to assess the frequency and predictors of hospitalization in patients with AF.
Methods: The ORBIT-AF registry is a prospective, observational study of outpatients with AF enrolled from June 29, 2010, to August 9, 2011. The current analysis included 9,484 participants with 1-year follow-up. Multivariable, logistic regression was used to identify baseline characteristics that were associated with first cause-specific hospitalization.
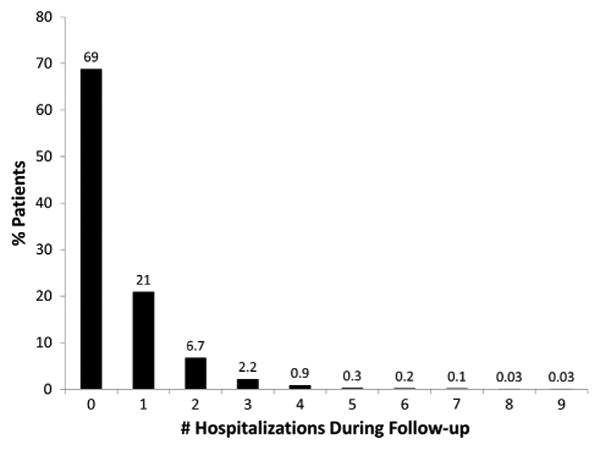
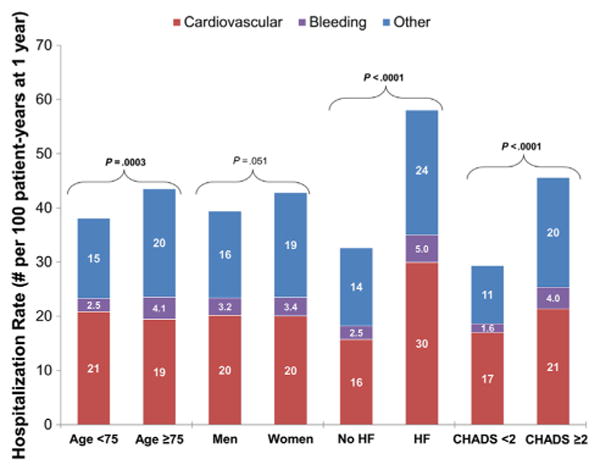
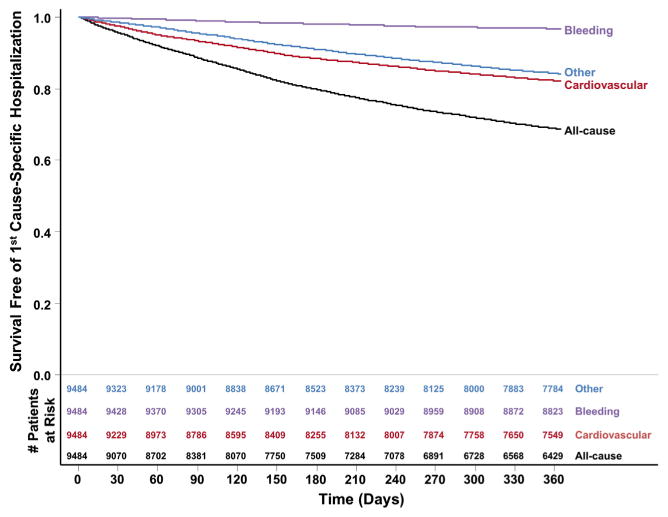
Results: Overall, 31% of patients with AF studied (n = 2,963) had 1 or more hospitalizations per year and 10% (n = 983) had 2 or more. The most common hospitalization cause was cardiovascular (20 per 100 patient-years vs 3.3 bleeding vs 17 noncardiovascular, nonbleeding). Compared with those not hospitalized, hospitalized patients were more likely to have concomitant heart failure (42% vs 28%, P < .0001), higher mean CHADS2 (1 point for congestive heart failure, hypertension, age ≥75, or diabetes; 2 points for prior stroke or transient ischemic attack) scores (2.5 vs 2.2, P < .0001), and more symptoms (baseline European Heart Rhythm Association class severe symptoms 18% vs 13%, P < .0001). In multivariable analysis, heart failure (adjusted hazard ratio [HR] 1.57 for New York Heart Association III/IV vs none, P < .0001), heart rate at baseline (adjusted HR 1.11 per 10-beats/min increase >66, P < .0001), and AF symptom class (adjusted HR 1.37 for European Heart Rhythm Association severe vs none, P < .0001) were the major predictors of incident hospitalization.
Conclusions: Hospitalization is common in outpatients with AF and is independently predicted by heart failure and AF symptoms. Improved symptom control, rate control, and comorbid condition management should be evaluated as strategies to reduce health care use in these patients.
Trial registration: ClinicalTrials.gov NCT01165710.
Copyright © 2014 Mosby, Inc. All rights reserved.
Figures
References
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285(18):2370–5. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22(8):983–8. - PubMed
-
- Benjamin EJ, Wolf PA, D'Agostino RB, et al. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98(10):946–52. - PubMed
-
- Coyne KS, Paramore C, Grandy S, et al. Assessing the direct costs of treating nonvalvular atrial fibrillation in the United States. Value Health. 2006;9(5):348–56. - PubMed
-
- Wu EQ, Birnbaum HG, Mareva M, et al. Economic burden and comorbidities of atrial fibrillation in a privately insured population. Curr Med Res Opin. 2005;21(10):1693–9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
