

Lung microbiome and disease progression in idiopathic pulmonary fibrosis: an analysis of the COMET study
- PMID: 24767767
- PMCID: PMC4142525
- DOI: 10.1016/S2213-2600(14)70069-4
Lung microbiome and disease progression in idiopathic pulmonary fibrosis: an analysis of the COMET study
Erratum in
- Lancet Respir Med. 2014 Aug;2(8):e14
Abstract
Background: The role of the lung microbiome in the pathogenesis of idiopathic pulmonary fibrosis is unknown. We investigated whether unique microbial signatures were associated with progression of idiopathic pulmonary fibrosis.
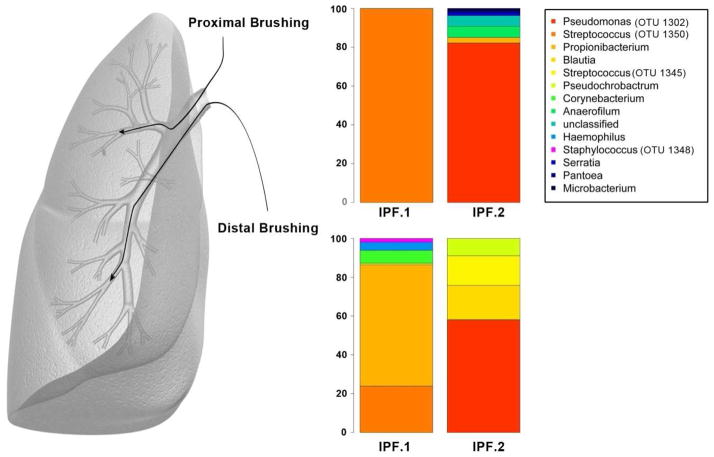
Methods: Patients (aged 35-80 years) with idiopathic pulmonary fibrosis within 4 years of diagnosis from the Correlating Outcomes with biochemical Markers to Estimate Time-progression (COMET) in idiopathic pulmonary fibrosis study were followed up for a maximum of 80 weeks. Progression-free survival was defined as time to death, acute exacerbation, lung transplant, or decrease in forced vital capacity (FVC) of 10% or greater or decrease in diffusion capacity of the lung (DLCO) of 15% or greater. DNA was isolated from 55 samples of bronchoscopic alveolar lavage. 454 pyrosequencing was used to assign operational taxonomic units (OTUs) to bacteria based on a 3% sequence divergence. Adjusted Cox models were used to identify OTUs that were significantly associated with progression-free survival at a p<0.10. These OTUs were then used in the analysis of the principal components. The association between principal components and microbes with high factor loadings and progression-free survival were assessed with Cox regression analyses. The COMET study is registered with ClinicalTrials.gov, number NCT01071707.
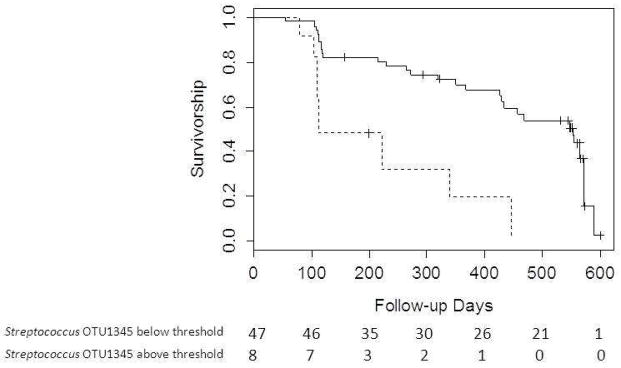
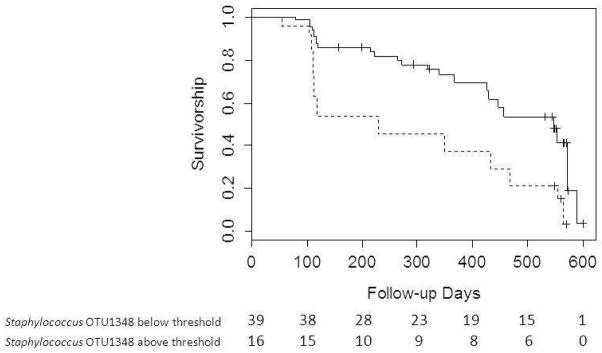
Findings: Mean FVC was 70.1% (SD 17.0) and DLCO 42.3% (14.0) of predicted. Disease progression was significantly associated with increased relative abundance of two OTUs-Streptococcus OTU 1345 (relative risk 1.11, 95% CI 1.04-1.18; p=0.0009) and Staphylococcus OTU 1348 (1.16, 1.03-1.31, p=0.012). Thresholds for relative abundance of each OTU associated with progression-free survival were more than 3.9% for Streptococcus OTU 1345 (10.19, 2.94-35.35; p=0.0002) and more than 1.8% for Staphylococcus OTU 1348 (5.06, 1.71-14.93; p=0.003).
Interpretation: These preliminary data suggest progression of idiopathic pulmonary fibrosis is associated with the presence of specific members within the Staphylococcus and Streptococcus genera. Additional research will be needed to identify the specific bacterial species and to ascertain whether this is a causal association.
Funding: National Institutes of Health.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflicts of Interest:
MH reports grants from NHLBI during the conduct of the study; grants and personal fees from GSK, personal fees from Pfizer, personal fees from BoehringerIngelheim, personal fees from Forest, personal fees from Novartis, personal fees from Medimmune, from Ikaria, personal fees from Regeneron, personal fees from Grifols, personal fees from Uptodate, outside the submitted work.
YZ, SM, and NT report grants from NIH during the conduct of this study.
IN reports grants from NIH during the conduct of the study. In addition, Dr. Noth has a patent TOLLIP SNPs in IPF pending.
VL and BM report no conflict of interest.
EW reports grants from the NIH during the conduct of this study.
KF reports personal fees and non-financial support from BoehringerIngelheim, during the conduct of the study; personal fees from BoehringerIngelheim, personal fees from Fibrogen, personal fees from Genentech, personal fees from Gilead, personal fees from Ikaria, personal fees from ImmuneWorks, personal fees from MedImmune, personal fees from Novartis, personal fees from Takeda, personal fees from Vertex, personal fees from Veracyte, personal fees from Roche, personal fees from Pulmonary Fibrosis Foundation, grants from ImmuneWorks, grants and personal fees from Intermune, grants from Bristol-Myers Squibb, personal fees from Glaxo Smith Klein, personal fees from Forest, personal fees from Up To Date, personal fees from NACE, personal fees from Excel, personal fees from France Foundation outside the submitted work.
GH reports reports grants from The National Institutes of Health during the conduct of the study.
FM reports grants from NHBLI, during the conduct of the study; personal fees from Able, personal fees from American Institute for Research, personal fees from Axon, personal fees from Grey Healthcare, personal fees from Merion, personal fees from Sudler& Hennessey, personal fees from Actelion, from Centocor, from Gilead, personal fees from Amgen, personal fees from Astra Zenneca, personal fees from Forest, personal fees from GSK, personal fees from Ikaria, personal fees from Jannsens, personal fees from Merck, personal fees from Nycomed/Takeda, personal fees from Pearl, personal fees from Pfizer, personal fees from Forest, personal fees from GSK, personal fees from Nycomed/Takeda, personal fees from American College of Chest Physicians, personal fees from Center for Healthcare Education, personal fees from CME Incite, personal fees from Inova, personal fees from MedScape/Web MD, personal fees from National Association for Continuing Education, personal fees from NCME, personal fees from Peer Voice, personal fees from Projects in Knowledge, personal fees from St. John's Hospital, personal fees from St. Mary's Hospital, personal fees from University of Illinois, Chicago, personal fees from University of Texas, Southwestern, personal fees from University of Virginia, personal fees from UpToDate, personal fees from Wayne State University, personal fees from Carden Jennings, personal fees from Ikaria, personal fees from MedImmune, personal fees from Nycomed/Takeda, personal fees from Vertex, personal fees and other from BoehringerIngelheim, personal fees from Bayer, personal fees from Forest, personal fees from GSK, personal fees from Nycomed/Takeda, personal fees from Prescott, personal fees from Informa, from Stromedix, from Promedior, personal fees from CSA Medical, personal fees from Miller Medical Communications, personal fees from Veracyte, outside the submitted work.
Figures
Comment in
-
Respiratory microbiome in IPF: cause, effect, or biomarker?Lancet Respir Med. 2014 Jul;2(7):511-3. doi: 10.1016/S2213-2600(14)70088-8. Epub 2014 Apr 21. Lancet Respir Med. 2014. PMID: 24767768 No abstract available.
-
The changing landscape of idiopathic pulmonary fibrosis.Lancet Respir Med. 2014 Jul;2(7):507. doi: 10.1016/S2213-2600(14)70146-8. Lancet Respir Med. 2014. PMID: 25008951 No abstract available.
References
-
- O'Dwyer DN, Armstrong ME, Trujillo G, et al. The Toll-like Receptor 3 L412F Polymorphism and Disease Progression in Idiopathic Pulmonary Fibrosis. Am J Respir Crit Care Med. 2013;188(12):1442–50. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
