

Cromolyn ameliorates acute and chronic injury in a rat lung transplant model
- PMID: 24768366
- PMCID: PMC4336160
- DOI: 10.1016/j.healun.2014.03.004
Cromolyn ameliorates acute and chronic injury in a rat lung transplant model
Abstract
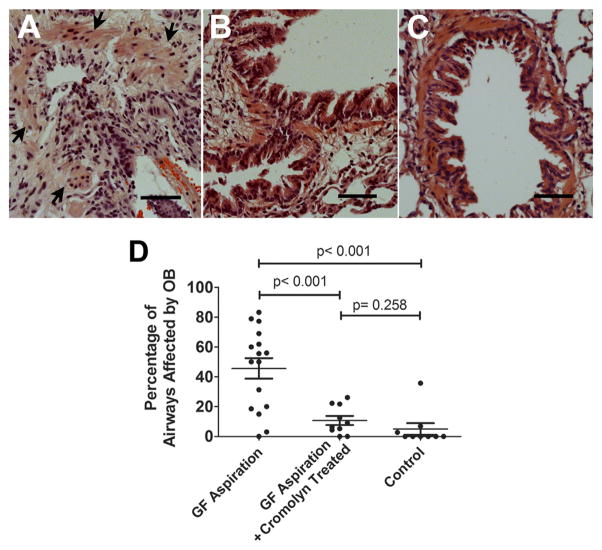
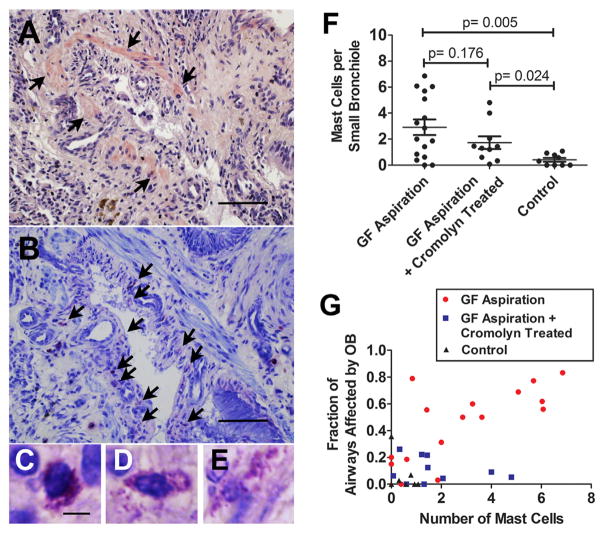
Background: Mast cells have been associated with obliterative bronchiolitis (OB) in human pulmonary allografts, although their role in the development of OB remains unknown.
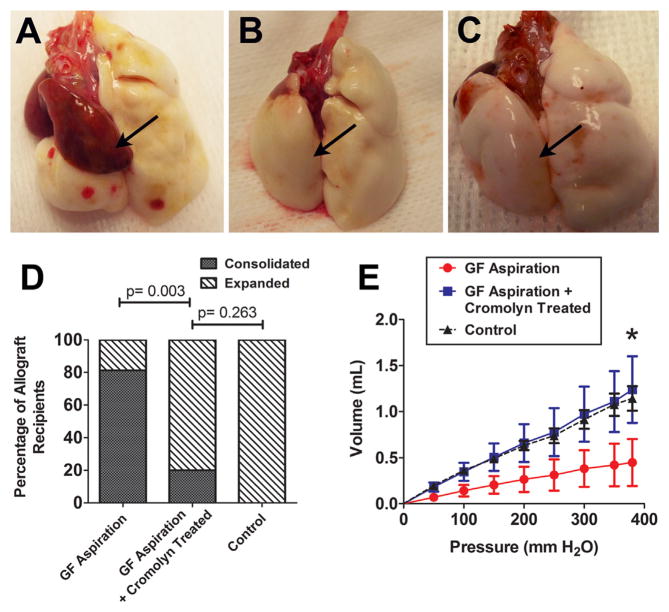
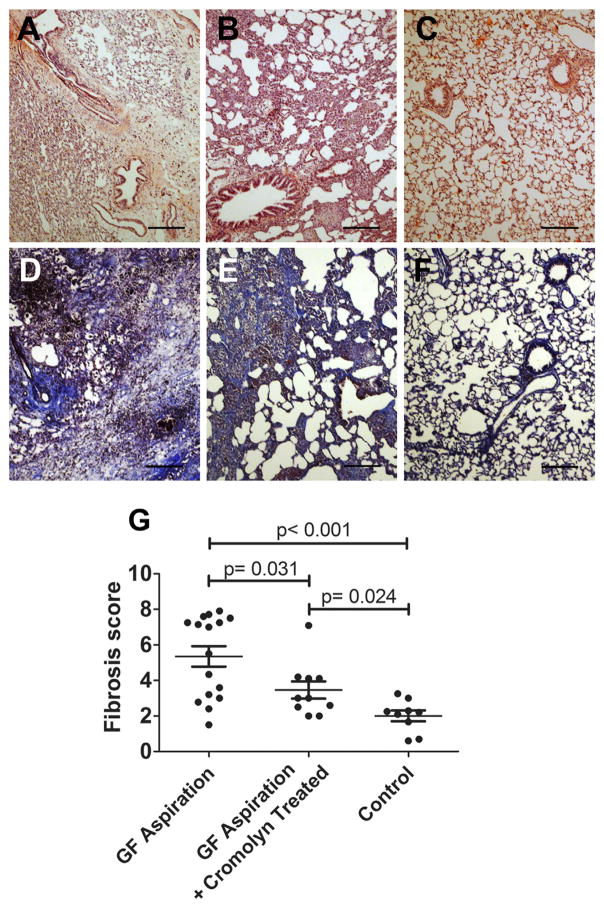
Methods: In this study, we evaluated the role of mast cells in pulmonary allograft rejection using an orthotopic rat pulmonary allograft model that utilizes chronic aspiration of gastric fluid to reliably obtain OB. Pulmonary allograft recipients (n = 35) received chronic aspiration of gastric fluid with (n = 10) and without (n = 16) treatment with a mast cell membrane stabilizer, cromolyn sodium, or chronic aspiration with normal saline (n = 9) as a control.
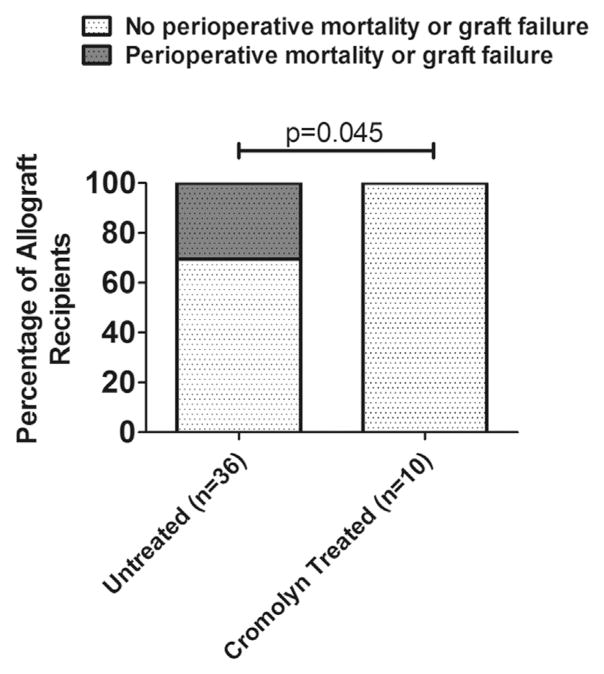
Results: The acute graft injury associated with long ischemic time in the model (6 hours total ischemic time; typical acute graft injury rate ~30%) was apparently blocked by cromolyn, because peri-operative mortality associated with the acute graft injury was not observed in any of the animals receiving cromolyn (p = 0.045). Further, the rats receiving cromolyn developed significantly fewer OB lesions than those treated with gastric fluid alone (p < 0.001), with a mean reduction of 46% of the airways affected.
Conclusions: These findings provide impetus for further studies aimed at elucidating the effects of cromolyn and the role of mast cells in pulmonary allotransplantation.
Keywords: aspiration; gastric fluid; mast cells; obliterative bronchiolitis; pulmonary allograft.
Copyright © 2014 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
