

Immunoglobulin and T cell receptor gene high-throughput sequencing quantifies minimal residual disease in acute lymphoblastic leukemia and predicts post-transplantation relapse and survival
- PMID: 24769317
- PMCID: PMC5259557
- DOI: 10.1016/j.bbmt.2014.04.018
Immunoglobulin and T cell receptor gene high-throughput sequencing quantifies minimal residual disease in acute lymphoblastic leukemia and predicts post-transplantation relapse and survival
Abstract
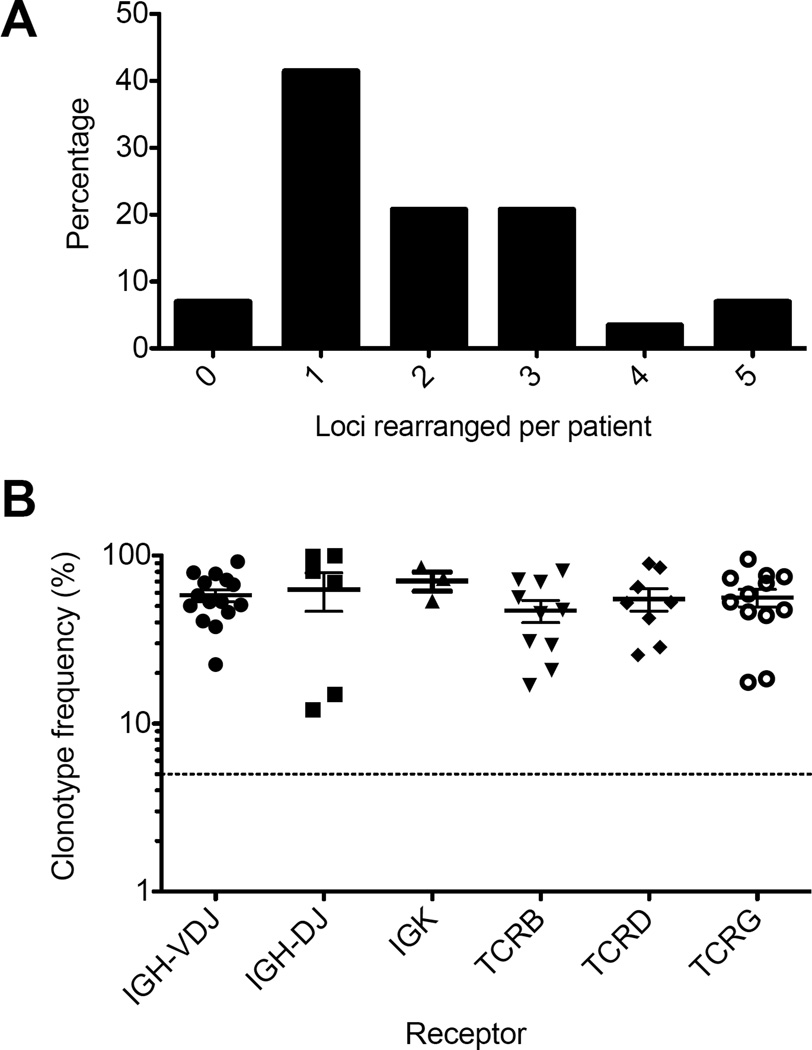
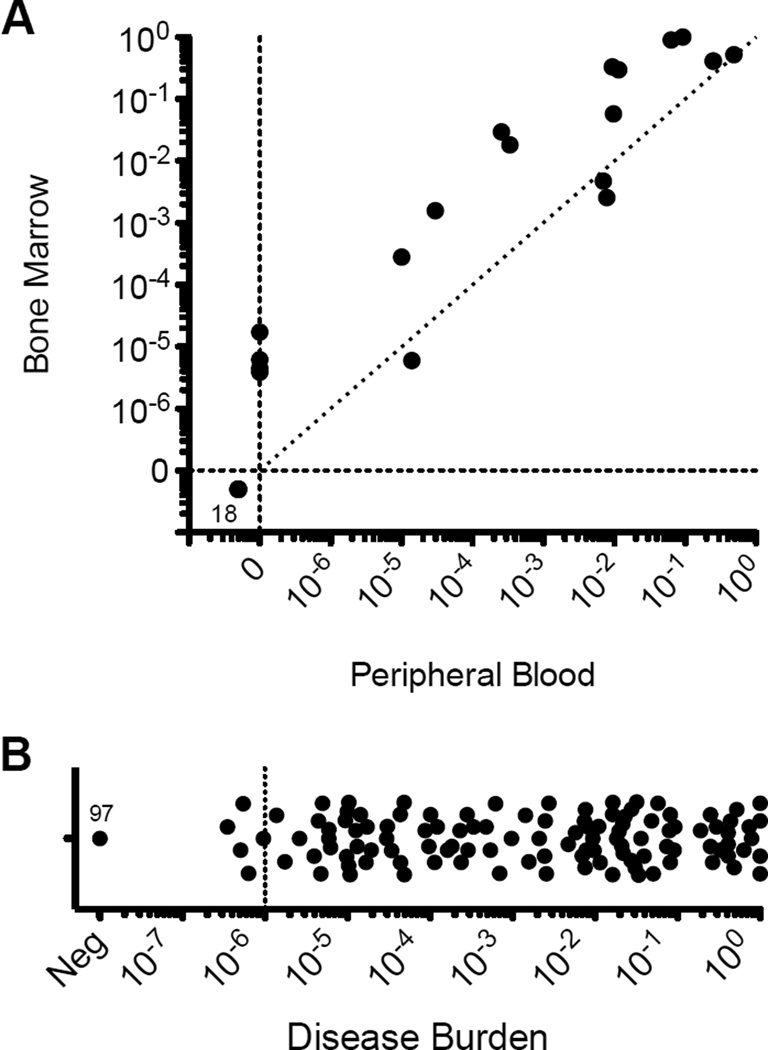
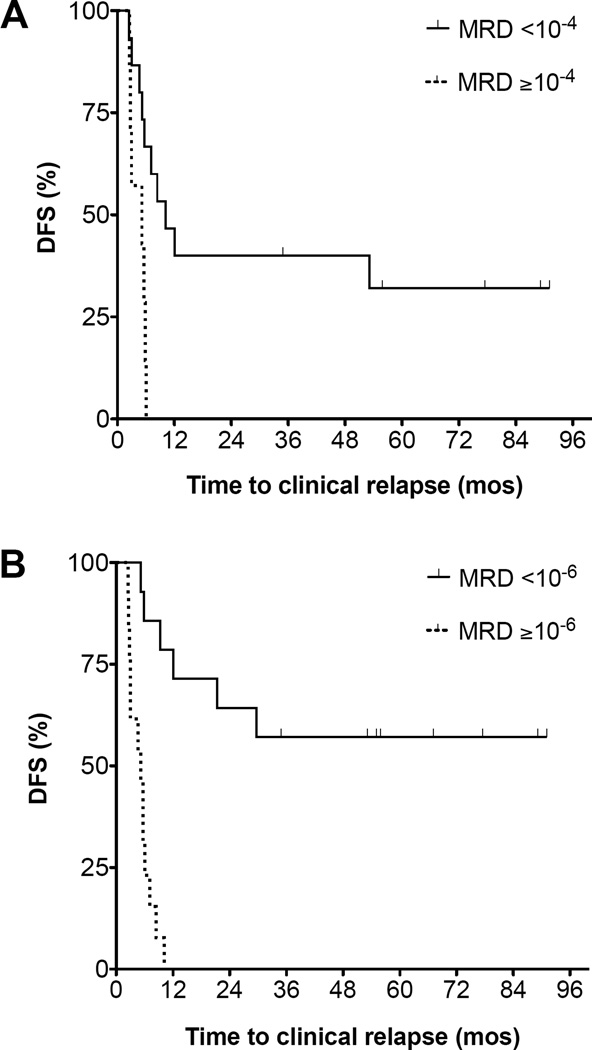
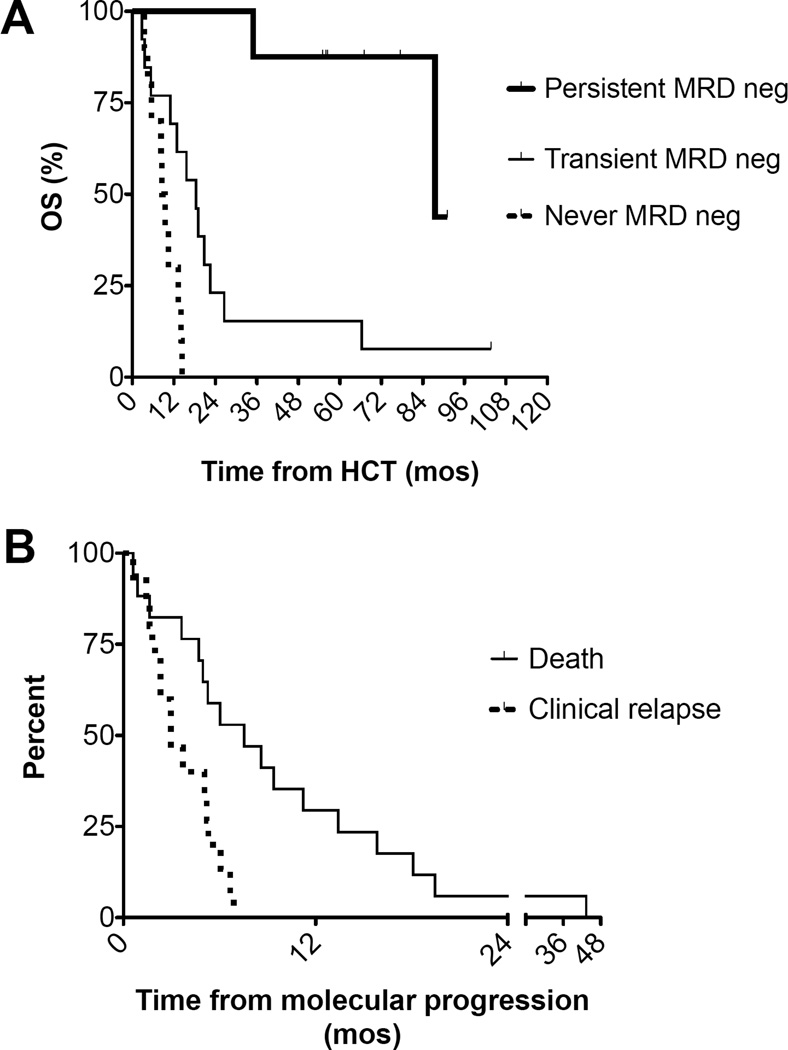
Minimal residual disease (MRD) quantification is an important predictor of outcome after treatment for acute lymphoblastic leukemia (ALL). Bone marrow ALL burden ≥ 10(-4) after induction predicts subsequent relapse. Likewise, MRD ≥ 10(-4) in bone marrow before initiation of conditioning for allogeneic (allo) hematopoietic cell transplantation (HCT) predicts transplantation failure. Current methods for MRD quantification in ALL are not sufficiently sensitive for use with peripheral blood specimens and have not been broadly implemented in the management of adults with ALL. Consensus-primed immunoglobulin (Ig), T cell receptor (TCR) amplification and high-throughput sequencing (HTS) permit use of a standardized algorithm for all patients and can detect leukemia at 10(-6) or lower. We applied the LymphoSIGHT HTS platform (Sequenta Inc., South San Francisco, CA) to quantification of MRD in 237 samples from 29 adult B cell ALL patients before and after allo-HCT. Using primers for the IGH-VDJ, IGH-DJ, IGK, TCRB, TCRD, and TCRG loci, MRD could be quantified in 93% of patients. Leukemia-associated clonotypes at these loci were identified in 52%, 28%, 10%, 35%, 28%, and 41% of patients, respectively. MRD ≥ 10(-4) before HCT conditioning predicted post-HCT relapse (hazard ratio [HR], 7.7; 95% confidence interval [CI], 2.0 to 30; P = .003). In post-HCT blood samples, MRD ≥10(-6) had 100% positive predictive value for relapse with median lead time of 89 days (HR, 14; 95% CI, 4.7 to 44, P < .0001). The use of HTS-based MRD quantification in adults with ALL offers a standardized approach with sufficient sensitivity to quantify leukemia MRD in peripheral blood. Use of this approach may identify a window for clinical intervention before overt relapse.
Keywords: Acute lymphoblastic leukemia; Allogeneic hematopoietic cell transplantation; High-throughput sequencing; Minimal residual disease; Next-generation sequencing.
Copyright © 2014 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Other authors report no potential conflicts of interest.
Figures
Comment in
-
Next generation MRD.Biol Blood Marrow Transplant. 2014 Sep;20(9):1259-60. doi: 10.1016/j.bbmt.2014.07.002. Epub 2014 Jul 10. Biol Blood Marrow Transplant. 2014. PMID: 25016196 Free PMC article. No abstract available.
References
-
- Bruggemann M, Gokbuget N, Kneba M. Acute lymphoblastic leukemia: monitoring minimal residual disease as a therapeutic principle. Semin. Oncol. 2012;39(1):47–57. - PubMed
-
- Bunin N, Johnston DA, Roberts WM, Ouspenskaia MV, Papusha VZ, Brandt MA, et al. Residual leukaemia after bone marrow transplant in children with acute lymphoblastic leukaemia after first haematological relapse or with poor initial presenting features. Br. J. Haematol. 2003;120(4):711–715. - PubMed
-
- Conter V, Bartram CR, Valsecchi MG, Schrauder A, Panzer-Grumayer R, Moricke A, et al. Molecular response to treatment redefines all prognostic factors in children and adolescents with B-cell precursor acute lymphoblastic leukemia: results in 3184 patients of the AIEOP-BFM ALL 2000 study. Blood. 2010;115(16):3206–3214. - PubMed
-
- Bader P, Hancock J, Kreyenberg H, Goulden NJ, Niethammer D, Oakhill A, et al. Minimal residual disease (MRD) status prior to allogeneic stem cell transplantation is a powerful predictor for post-transplant outcome in children with ALL. Leukemia. 2002;16(9):1668–1672. - PubMed
-
- Knechtli CJ, Goulden NJ, Hancock JP, Grandage VL, Harris EL, Garland RJ, et al. Minimal residual disease status before allogeneic bone marrow transplantation is an important determinant of successful outcome for children and adolescents with acute lymphoblastic leukemia. Blood. 1998;92(11):4072–4079. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
