

Pathological function of Ca2+-sensing receptor in pulmonary arterial hypertension
- PMID: 24770445
- PMCID: PMC5137257
- DOI: 10.1540/jsmr.50.8
Pathological function of Ca2+-sensing receptor in pulmonary arterial hypertension
Abstract
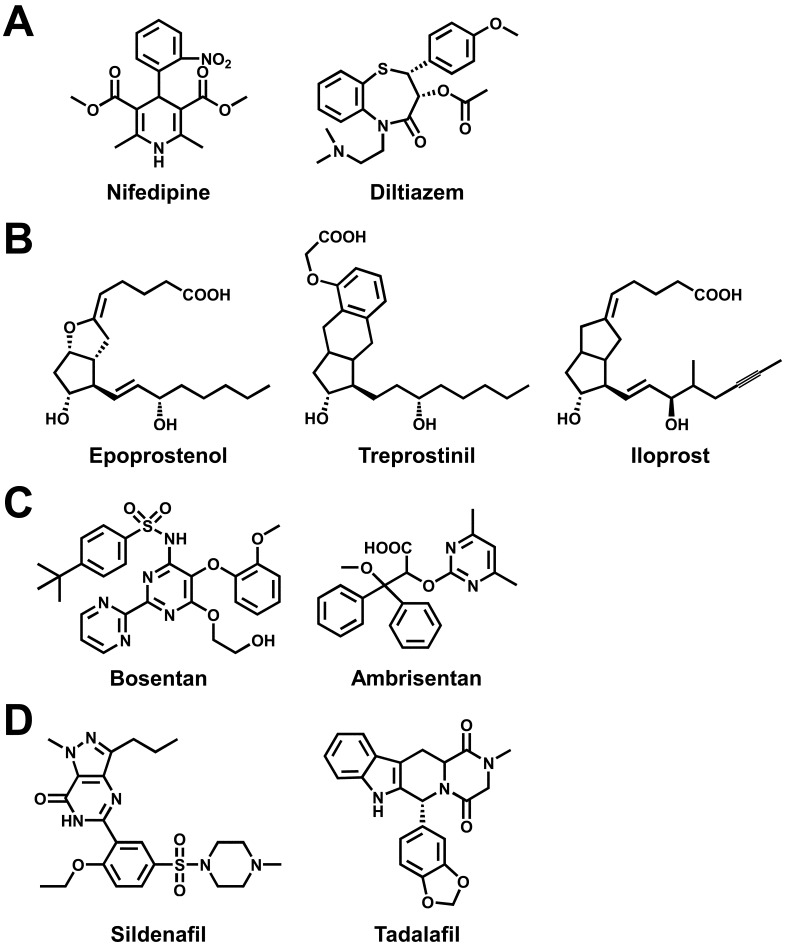
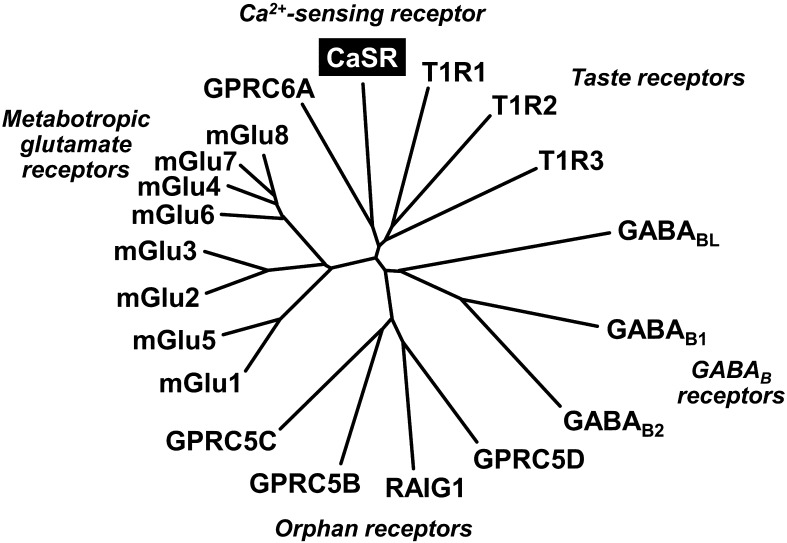
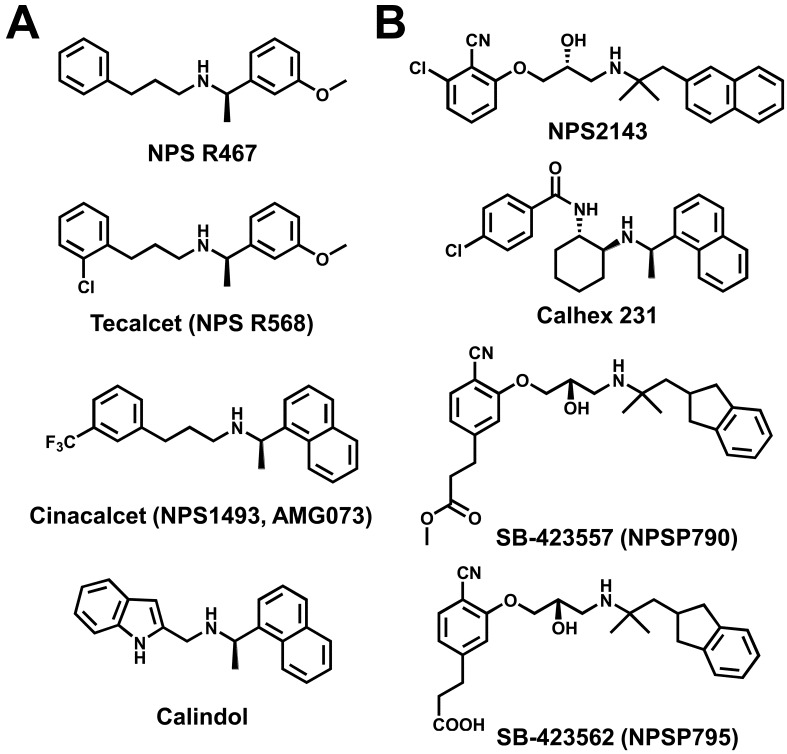
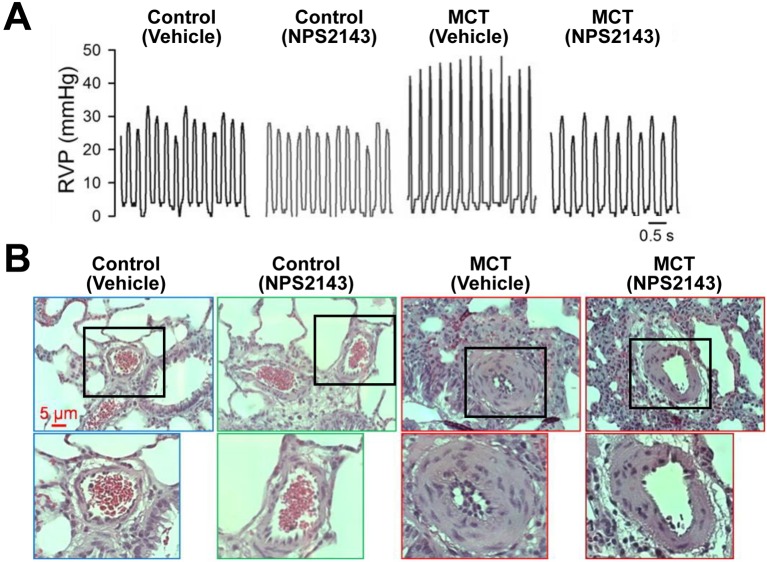
Pulmonary arterial hypertension (PAH) is defined as an intractable disease characterized by a progressive elevation of pulmonary vascular resistance (PVR) and pulmonary arterial pressure (PAP), leading to right heart failure and premature death. The five-year survival rate after diagnosis is approximately 57%. Although extensive research has identified some factors associated with the cause of PAH, the etiology and pathogenesis remain unclear. In addition to Ca(2+) channel blockers (nifedipine, diltiazem), three categories of drug have been developed for the treatment of PAH based on the pathological mechanisms: prostacyclin and its analogues (epoprostenol, treprostinil, iloprost), endothelin receptor antagonists (bosentan, ambrisentan), and phosphodiesterase type 5 inhibitors (sildenafil, tadalafil). However, screening of novel types of drug acting on the signal pathway associated with the pathological mechanism underlying PAH is ongoing. We recently found that the extracellular Ca(2+)-sensing receptor (CaSR), which belongs to family C of the G protein-coupled receptor (GPCR) superfamily, is upregulated in pulmonary arterial smooth muscle cells (PASMCs) from patients with idiopathic PAH (IPAH). The upregulated CaSR is necessary for the enhanced Ca(2+) signaling and the augmented cell proliferation in PASMCs from IPAH patients. Most importantly, blockage of CaSR with an antagonist, NPS2143, prevents the development of pulmonary hypertension and right ventricular hypertrophy in animal models of pulmonary hypertension. The use of calcilytics, antagonists of CaSR, may be a novel therapeutic approach for PAH patients.
Figures

References
-
- Rich S, Dantzker DR, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Koerner SK, Levy PC, Reid LM, Vreim CE, Williams GW. Primary pulmonary hypertension. A national prospective study. Ann Intern Med. 1987; 107(2): 216–23. doi: 10.7326/0003-4819-107-2-216 - DOI - PubMed
-
- Badesch DB, Raskob GE, Elliott CG, Krichman AM, Farber HW, Frost AE, Barst RJ, Benza RL, Liou TG, Turner M, Giles S, Feldkircher K, Miller DP, McGoon MD. Pulmonary arterial hypertension: baseline characteristics from the REVEAL Registry. Chest. 2010; 137(2): 376–87. doi: 10.1378/chest.09-1140 - DOI - PubMed
-
- Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, Elliott CG, Gaine SP, Gladwin MT, Jing ZC, Krowka MJ, Langleben D, Nakanishi N, Souza R. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009; 54 (1 Suppl): S43–54. doi: 10.1016/j.jacc.2009.04.012 - DOI - PubMed
-
- Yu Y, Fantozzi I, Remillard CV, Landsberg JW, Kunichika N, Platoshyn O, Tigno DD, Thistlethwaite PA, Rubin LJ, Yuan JX. Enhanced expression of transient receptor potential channels in idiopathic pulmonary arterial hypertension. Proc Natl Acad Sci USA. 2004; 101(38): 13861–6. doi: 10.1073/pnas.0405908101 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous