

[Performance of the Pediatric Index of Mortality 2 in a pediatric intensive care unit]
- PMID: 24770688
- PMCID: PMC4031884
- DOI: 10.5935/0103-507x.20140007
[Performance of the Pediatric Index of Mortality 2 in a pediatric intensive care unit]
Abstract
Objective: To assess the discrimination and calibration of the Pediatric Index of Mortality 2 in patients admitted to a pediatric intensive care unit.
Methods: The study was conducted with a contemporary cohort from November 2005 to November 2006. Patients aged 29 days to 18 years were included in the study. Patients who died within 12 hours of admission and cases of readmission were excluded from the study. The performance of the Pediatric Index of Mortality 2 was assessed by means of the Hosmer-Lemeshow goodness-of-fit test, the standardized mortality ratio and the area under receiver operating characteristic (ROC) curve with 95% confidence interval. The significance level was established as 5%.
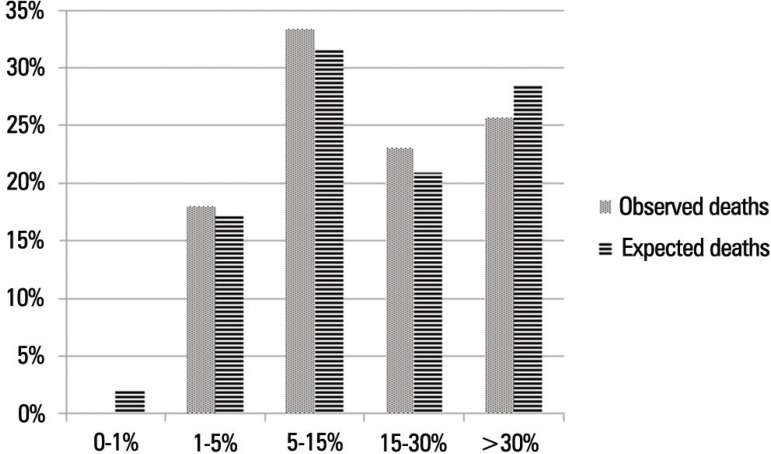
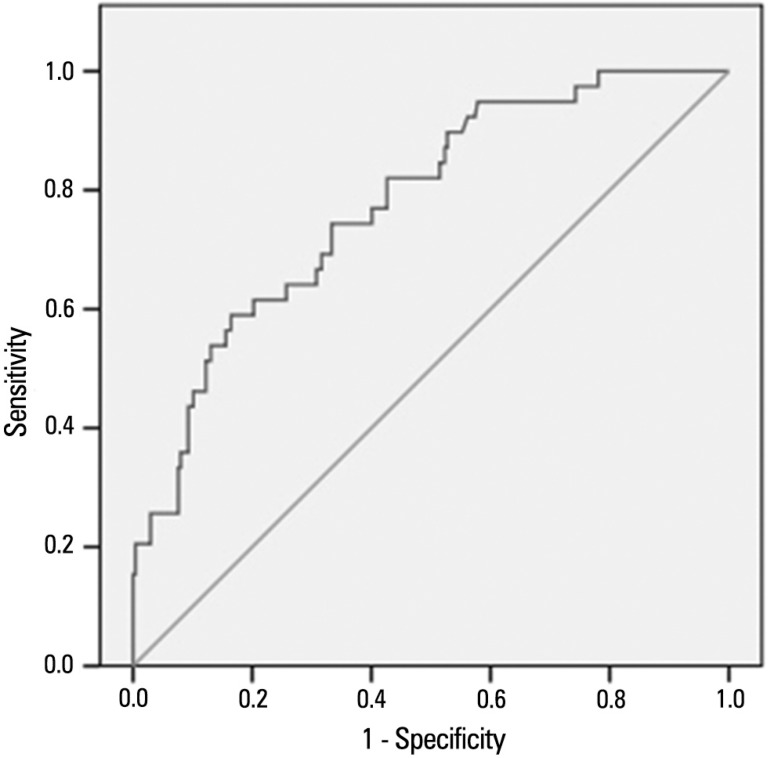
Results: A total of 276 admissions to the pediatric intensive care unit were included in the analysis. The mortality rate was 14.13%, and the efficiency of admission 0.88%. The median age of the sample was 42.22 months, and most participants were male (60.1%). Most admissions were referrals from the emergency department. The mean duration of stay in pediatric intensive care unit was 6.43±5.23 days. Approximately 72.46% of admissions were for clinical reasons and exhibited an association with the outcome death (odds ratio: 2.9; 95%CI: 1.09-7.74; p=0.017). Calibration of the Pediatric Index of Mortality 2 with the chi-square statistic was 12.2686 (p=0.1396) in the Hosmer-Lemeshow goodness-of-fit test, and the standardized mortality ratio was 1.0. The area under the ROC curve assessing model discrimination was 0.778.
Conclusion: Pediatric Index of Mortality 2 exhibited satisfactory performance.
Conflict of interest statement
Figures
References
-
- Cútulo LR, Furtado JR, Júnior, Botelho L. Perfil dos pacientes internados na unidade de terapia intensiva pediátrica do Hospital Infantil Joana de Gusmão no Ano de 1993. ACM Arq Catarin Med. 1994;23(2):95–100.
-
- Chalfin DB, Cohen IL, Lambrinos J. The economics and cost-effectiveness of critical care medicine. Intensive Care Med. 1995;21(11):952–961. Review. - PubMed
-
- Pollack MM, Ruttimann UE, Getson PR. Pediatric risk of mortality (PRISM) score. Crit Care Med. 1988;16(11):1110–1116. - PubMed
-
- Pollack MM, Patel KM, Ruttimann UE. PRISM III: an updated Pediatric Risk of Mortality score. Crit Care Med. 1996;24(5):743–752. - PubMed
-
- Shann F, Pearson G, Slater A, Wilkinson K. Paediatric index of mortality(PIM): a mortality prediction model for children in intensive care. Intensive Care Med. 1997;23(2):201–207. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
