

Improving anticoagulation in atrial fibrillation: observational study in three primary care trusts
- PMID: 24771841
- PMCID: PMC4001131
- DOI: 10.3399/bjgp14X679705
Improving anticoagulation in atrial fibrillation: observational study in three primary care trusts
Abstract
Background: Atrial fibrillation (AF) is a cause of stroke, and undertreatment with anticoagulants is a persistent issue despite their effectiveness.
Aim: To increase the proportion of people with AF treated appropriately using anticoagulants, and reduce inappropriate antiplatelet therapy.
Design of study: Cross-sectional analysis.
Setting: Electronic patient health records on 4604 patients with AF obtained from general practices in three inner London primary care trusts between April 2011 and 2013.
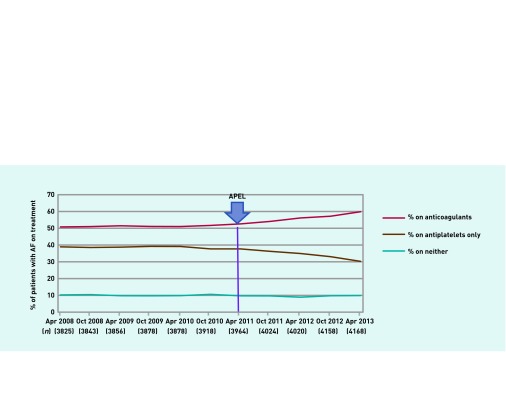
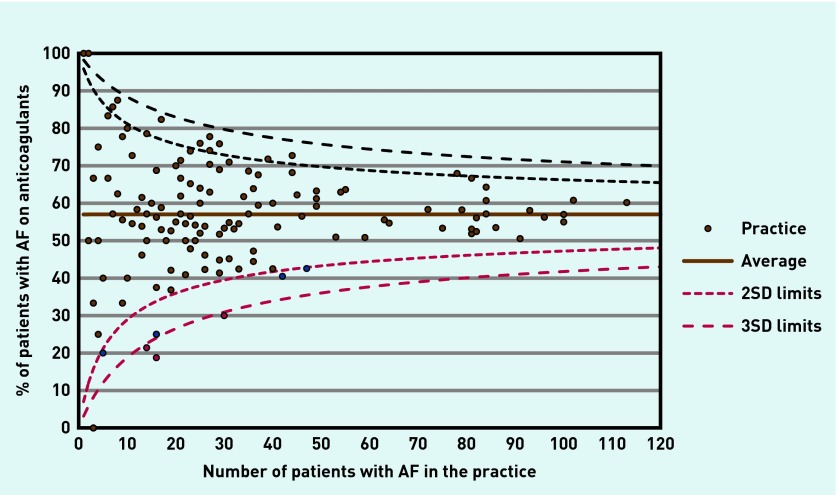
Method: The Anticoagulant Programme East London (APEL) sought to achieve its aims through an intervention with three components: altering professional beliefs using new clinical guidance and related education; facilitating change using computer software to support clinical decisions and patient review optimising anticoagulation; motivating change through evaluative feedback showing individual practice performance relative to peers.
Results: From April 2011 to April 2013, the proportion of people with CHA2DS2-VASc ≥1 on anticoagulants increased from 52.6% to 59.8% (trend difference P<0.001). The proportion of people with CHA2DS2-VASc ≥1 on aspirin declined from 37.7% to 30.3% (trend difference P<0.001). Comparing the 2 years before the intervention with the 2 years after, numbers of new people on the AF register almost doubled from 108 to 204.
Conclusions: The APEL programme supports improvement in clinical managing AF by a combined programme of education around agreed guidance, computer aids to facilitate decision-making and patient review and feedback of locally identifiable results. If replicated nationally over 3 years, such a programme could result in approximately 1600 fewer strokes every year.
Keywords: anticoagulants; atrial fibrillation; clinical decision support systems; patterns; prescribing; primary health care; stroke.
Figures
References
-
- Heeringa J, van der Kuip DA, Hofman A, et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J. 2006;27(8):949–953. - PubMed
-
- Mathur R, Pollara E, Hull S, et al. Ethnicity and stroke risk in patients with atrial fibrillation. Heart. 2013;99:1087–1092. - PubMed
-
- QStroke 2013. Risk calculator: http://qstroke.org (accessed 6 Mar 2014).
-
- QRisk2 2013. Risk calculator: http://qrisk.org (accessed 6 Mar 2014).
-
- Camm AJ, Lip YHG, De Caterina R, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with with the special contribution of the European Heart Rhythm Association. Eur Heart J. 2012;33(21):2719–2747. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous