

Dysphagia in the elderly
Abstract
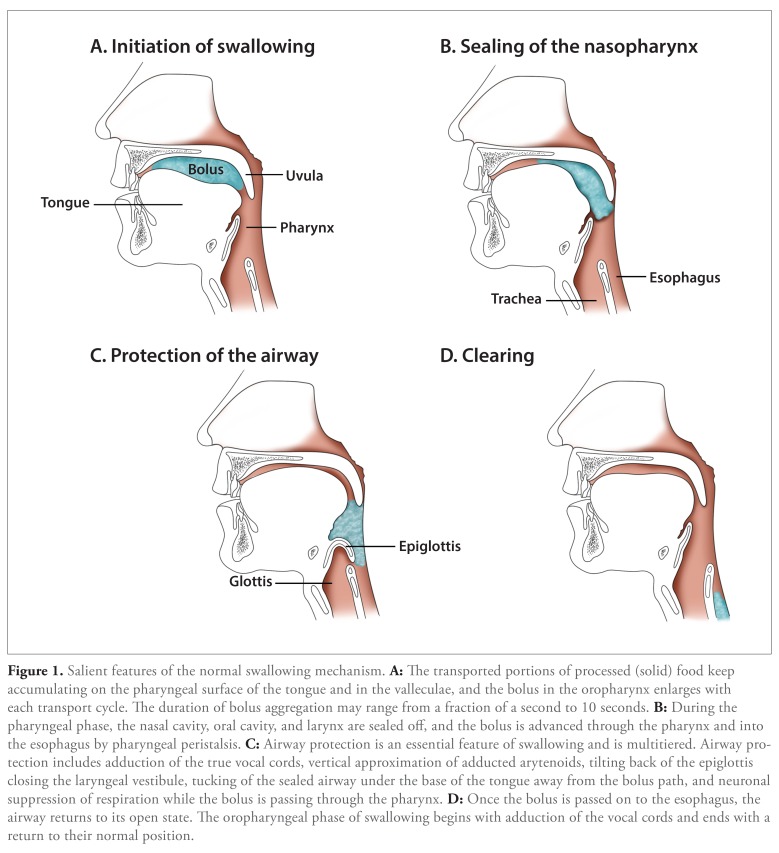
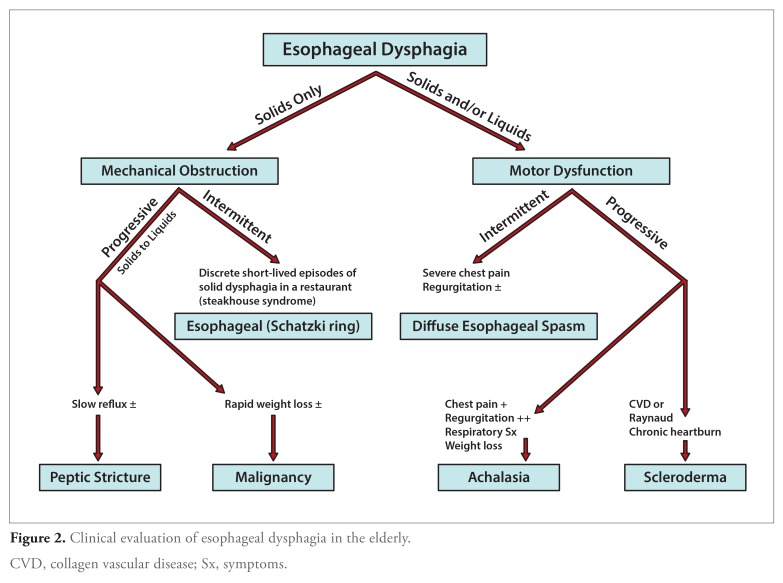
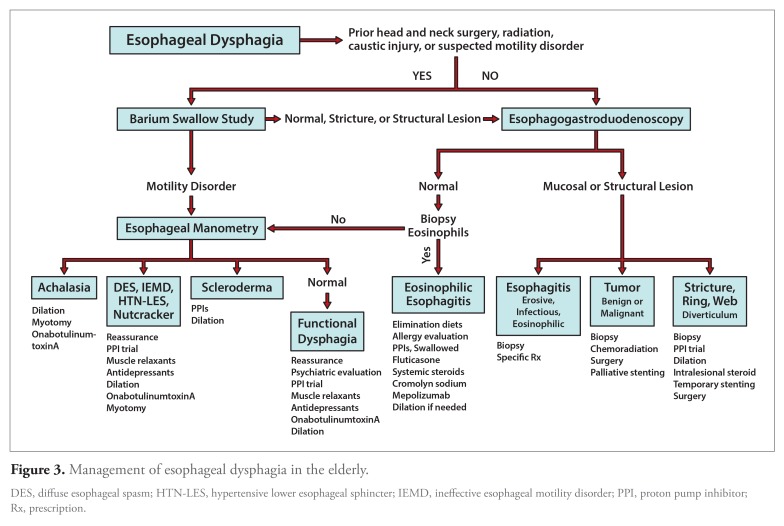
Elderly patients are inherently predisposed to dysphagia predominately because of comorbid health conditions. With the aging of the population in the United States, along with the increased prevalence of obesity and gastroesophageal reflux disease, healthcare providers will increasingly encounter older patients with either oropharyngeal or esophageal disease and complaints of dysphagia. Useful tests to evaluate dysphagia include the videofluoroscopic swallowing study and the fiberoptic endoscopic evaluation of swallowing. Swallow rehabilitation is useful to help patients compensate for swallowing difficulty and ultimately help strengthen the neuromusculature involved in swallowing.
Keywords: Esophageal dysphagia; aging; fiberoptic endoscopic evaluation of swallowing; oropharyngeal dysphagia; swallow function; videofluoroscopic swallowing study.
Figures
References
-
- Talley NJ, Weaver AL, Zinsmeister AR, Melton LJ., III Onset and disappearance of gastrointestinal symptoms and functional gastrointestinal disorders. Am J Epidemiol. 1992;136(2):165–177. - PubMed
-
- Cook IJ, Kahrilas PJ. AGA technical review on management of oropharyngeal dysphagia. Gastroenterology. 1999;116(2):455–478. - PubMed
-
- Lindgren S, Janzon L. Prevalence of swallowing complaints and clinical findings among 50-79-year-old men and women in an urban population. Dysphagia. 1991;6(4):187–192. - PubMed
-
- Barczi SR, Sullivan PA, Robbins J. How should dysphagia care of older adults differ? Establishing optimal practice patterns. Semin Speech Lang. 2000;21(4):347–361. - PubMed
-
- Siebens H, Trupe E, Siebens A, et al. Correlates and consequences of eating dependency in institutionalized elderly. J Am Geriatr Soc. 1986;34(3):192–198. - PubMed
LinkOut - more resources
Full Text Sources