

Branchial anomalies: diagnosis and management
- PMID: 24772172
- PMCID: PMC3960728
- DOI: 10.1155/2014/237015
Branchial anomalies: diagnosis and management
Abstract
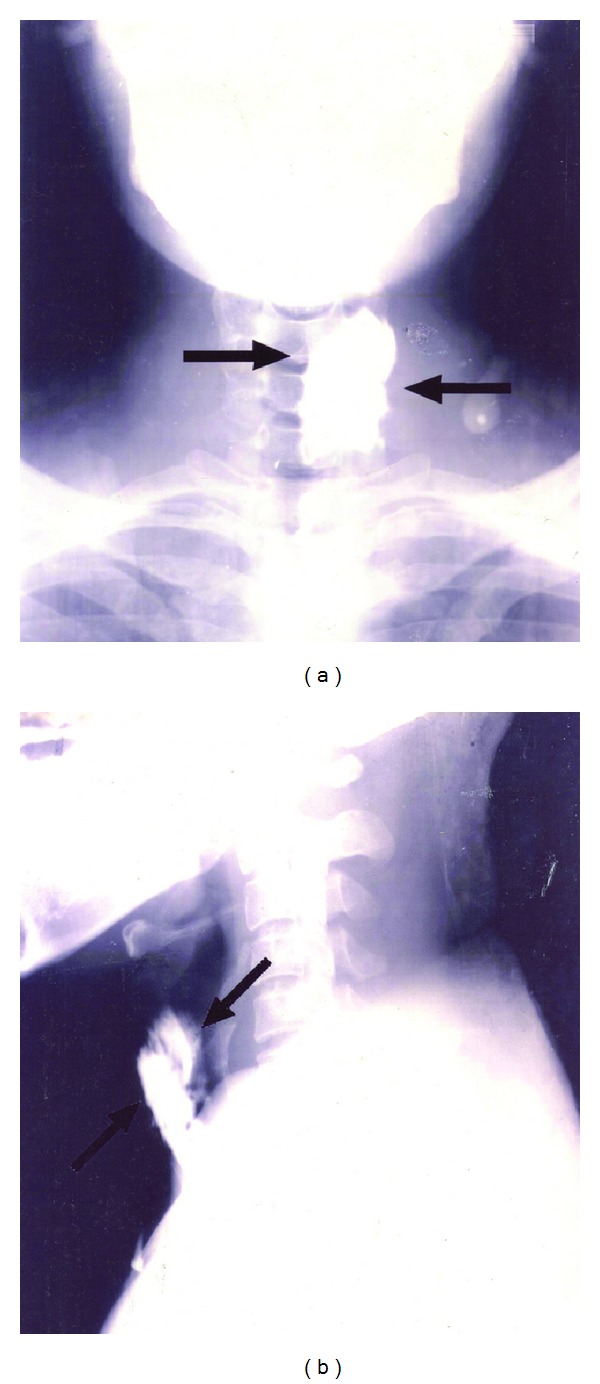
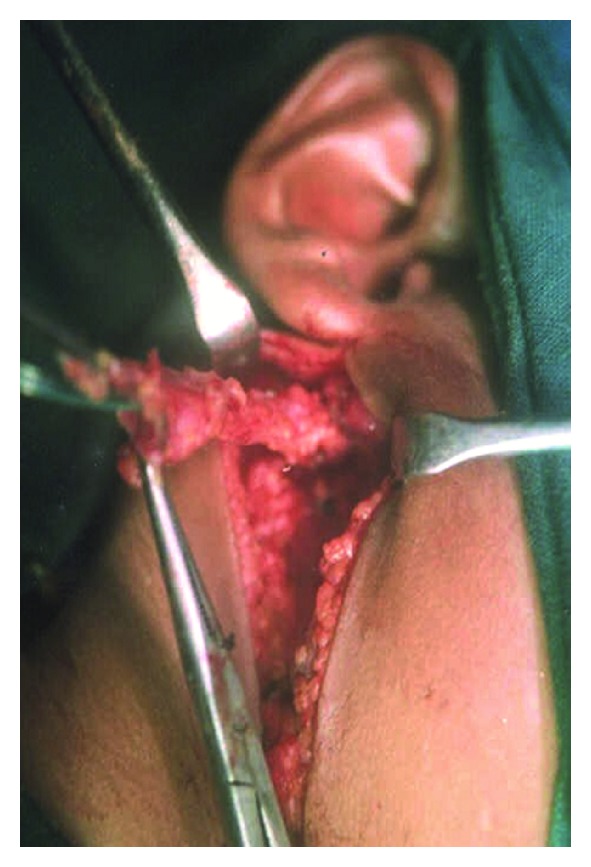
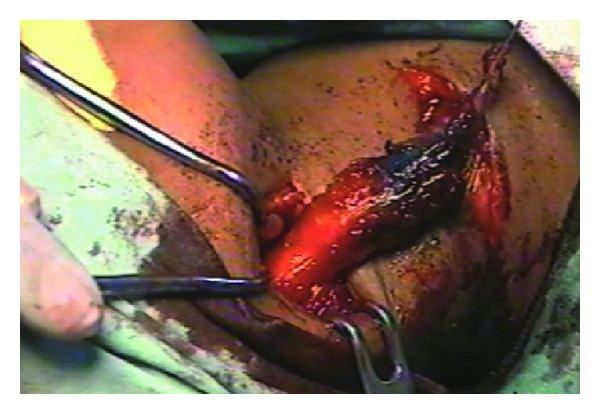
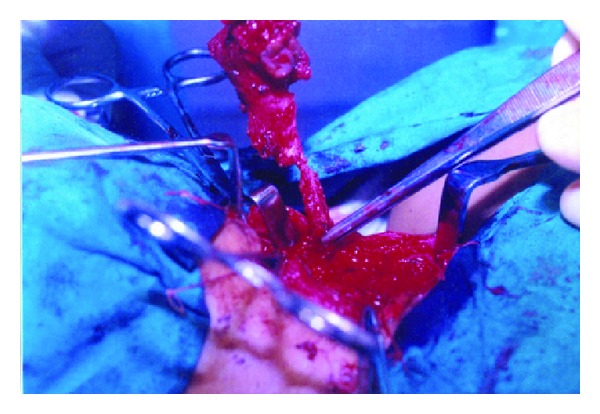
Objective. To find out the incidence of involvement of individual arches, anatomical types of lesions, the age and sex incidence, the site and side of predilection, the common clinical features, the common investigations, treatment, and complications of the different anomalies. Setting. Academic Department of Otolaryngology, Head and Neck Surgery. Design. A 10 year retrospective study. Participants. 30 patients with clinically proven branchial anomalies including patients with bilateral disease totaling 34 lesions. Main Outcome Measures. The demographical data, clinical features, type of branchial anomalies, and the management details were recorded and analyzed. Results and Observations. The mean age of presentation was 18.67 years. Male to female sex ratio was 1.27 : 1 with a male preponderance. Of the 34 lesions, maximum incidence was of second arch anomalies (50%) followed by first arch. We had two cases each of third and fourth arch anomalies. Only 1 (3.3%) patients of the 30 presented with lesion at birth. The most common pathological type of lesions was fistula (58.82%) followed by cyst. 41.18% of the lesions occurred on the right side. All the patients underwent surgical excision. None of our patients had involvement of facial nerve in first branchial anomaly. All patients had tracts going superficial to the facial nerve. Conclusion. Confirming the extent of the tract is mandatory before any surgery as these lesions pass in relation to some of the most vital structures of the neck. Surgery should always be the treatment option. injection of dye, microscopic removal and inclusion of surrounding tissue while excising the tract leads to a decreased incidence of recurrence.
Figures

Similar articles
-
Importance and Impact of Appropriate Radiology in the Management of Branchial Cleft Anomalies.Indian J Otolaryngol Head Neck Surg. 2019 Oct;71(Suppl 1):953-959. doi: 10.1007/s12070-019-01634-w. Epub 2019 Mar 23. Indian J Otolaryngol Head Neck Surg. 2019. PMID: 31742101 Free PMC article.
-
Second Branchial Anomalies: A Study of 94 Cases.Indian J Otolaryngol Head Neck Surg. 2017 Dec;69(4):540-543. doi: 10.1007/s12070-017-1195-1. Epub 2017 Sep 13. Indian J Otolaryngol Head Neck Surg. 2017. PMID: 29238688 Free PMC article.
-
Branchial anomalies in children.Int J Pediatr Otorhinolaryngol. 2011 Aug;75(8):1020-3. doi: 10.1016/j.ijporl.2011.05.008. Epub 2011 Jun 15. Int J Pediatr Otorhinolaryngol. 2011. PMID: 21680029
-
Management of congenital fourth branchial arch anomalies: a review and analysis of published cases.J Pediatr Surg. 2009 Jul;44(7):1432-9. doi: 10.1016/j.jpedsurg.2008.12.001. J Pediatr Surg. 2009. PMID: 19573674 Review.
-
Fourth branchial complex anomalies: a case series.Int J Pediatr Otorhinolaryngol. 2003 Nov;67(11):1227-33. doi: 10.1016/j.ijporl.2003.07.015. Int J Pediatr Otorhinolaryngol. 2003. PMID: 14597375 Review.
Cited by
-
Management of hypoparathyroidism in pregnancy and lactation - A report of 10 cases.Bone Rep. 2015 Jun 30;3:15-19. doi: 10.1016/j.bonr.2015.05.005. eCollection 2015 Dec. Bone Rep. 2015. PMID: 28377963 Free PMC article.
-
Midline Anterior Neck Inclusion Cyst in a Pediatric Patient: A Case Report and Literature Review with a Dermatologic Perspective.Medicina (Kaunas). 2025 Jan 2;61(1):64. doi: 10.3390/medicina61010064. Medicina (Kaunas). 2025. PMID: 39859047 Free PMC article. Review.
-
Possible Estrogen Dependency in the Pathogenesis of Branchial Cleft Cysts.Biomed Res Int. 2017;2017:1807056. doi: 10.1155/2017/1807056. Epub 2017 Dec 19. Biomed Res Int. 2017. PMID: 29410959 Free PMC article.
-
Perioperative Outcomes of Branchial Cleft Sinus Tract Excision in Pediatric Patients Without the Use of Intraoperative Dye.Ann Otol Rhinol Laryngol. 2025 Apr;134(4):245-248. doi: 10.1177/00034894241303021. Epub 2024 Nov 29. Ann Otol Rhinol Laryngol. 2025. PMID: 39614624 Free PMC article.
-
A fatal case of severe neck abscess due to a third branchial cleft fistula: morphologic and immunohistochemical analyses.Diagn Pathol. 2016 Sep 15;11(1):87. doi: 10.1186/s13000-016-0540-0. Diagn Pathol. 2016. PMID: 27628180 Free PMC article.
References
-
- Choi SS, Zalzal GH. Branchial anomalies: a review of 52 cases. Laryngoscope. 1995;105(9, part 1):909–913. - PubMed
-
- Kenealy JF, Torsiglieri AJ, Jr., Tom LW. Branchial cleft anomalies: a five-year retrospective review. Transactions of the Pennsylvania Academy of Ophthalmology and Otolaryngology. 1990;42:1022–1025. - PubMed
-
- Ford GR, Balakrishnan A, Evans JNG, Bailey CM. Branchial cleft and pouch anomalies. Journal of Laryngology and Otology. 1992;106(2):137–143. - PubMed
-
- Bajaj Y, Ifeacho S, Tweedie D, et al. Branchial anomalies in children. International Journal of Pediatric Otorhinolaryngology. 2011;75(8):1020–1023. - PubMed
-
- Reiter D. Third branchial cleft sinus: an unusual cause of neck abscess. International Journal of Pediatric Otorhinolaryngology. 1982;4(2):181–186. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
