

Molecular phenotypes of human parvovirus B19 in patients with myocarditis
- PMID: 24772258
- PMCID: PMC3999338
- DOI: 10.4330/wjc.v6.i4.183
Molecular phenotypes of human parvovirus B19 in patients with myocarditis
Abstract
Aim: To investigate molecular phenotypes of myocardial B19V-infection to determine the role of B19V in myocarditis and dilated cardiomyopathy (DCM).
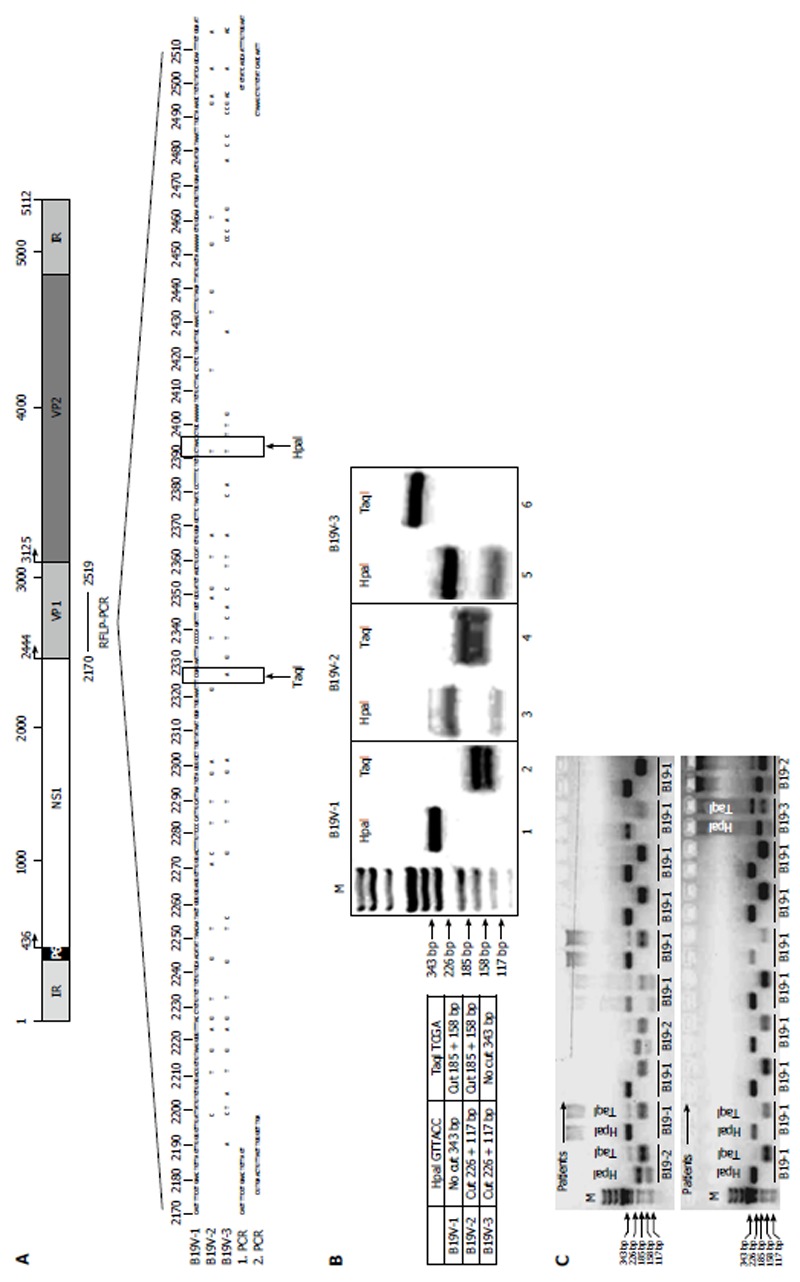
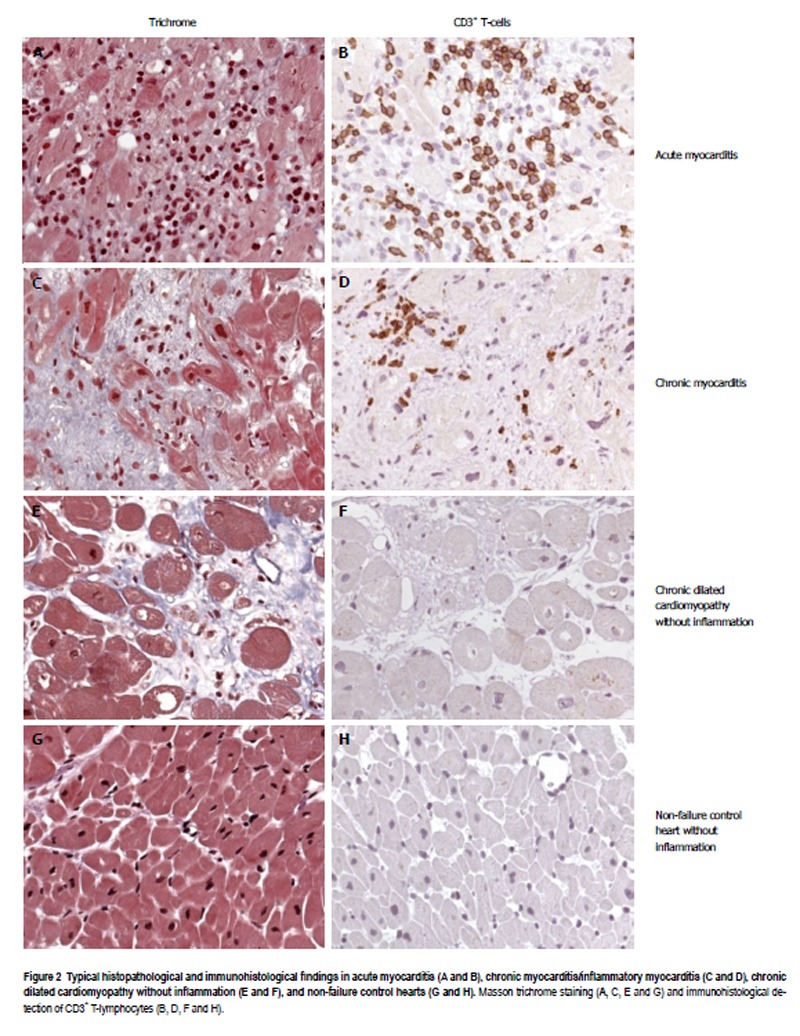
Methods: Endomyocardial biopsies (EMBs) from 498 B19V-positive patients with myocarditis and DCM were analyzed using molecular methods and functional experiments. EMBs were obtained from the University Hospitals of Greifswald and Tuebingen and additionally from 36 German cardiology centers. Control tissues were obtained at autopsy from 34 victims of accidents, crime or suicide. Identification of mononuclear cell infiltrates in EMBs was performed using immunohistological staining. Anti-B19V-IgM and anti-B19V-IgG were analyzed by enzyme-linked immunosorbent assay (ELISA). B19V viral loads were determined using in-house quantitative real-time polymerase chain reaction (PCR). For B19V-genotyping a new B19V-genotype-specific restriction fragment length polymorphism (RFLP)-PCR was established. B19V-genotyping was verified by direct DNA-sequencing and sequences were aligned using BLAST and BioEdit software. B19V P6-promoter and HHV6-U94-transactivator constructs were generated for cell culture experiments. Transfection experiments were conducted using human endothelial cells 1. Luciferase reporter assays were performed to determine B19V-replication activity. Statistical analysis and graphical representation were calculated using SPSS and Prism5 software.
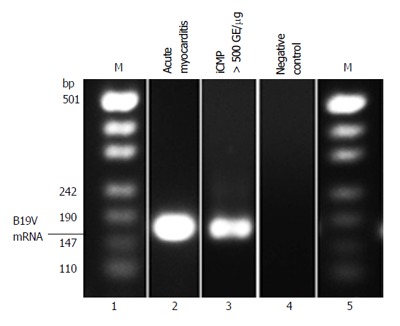
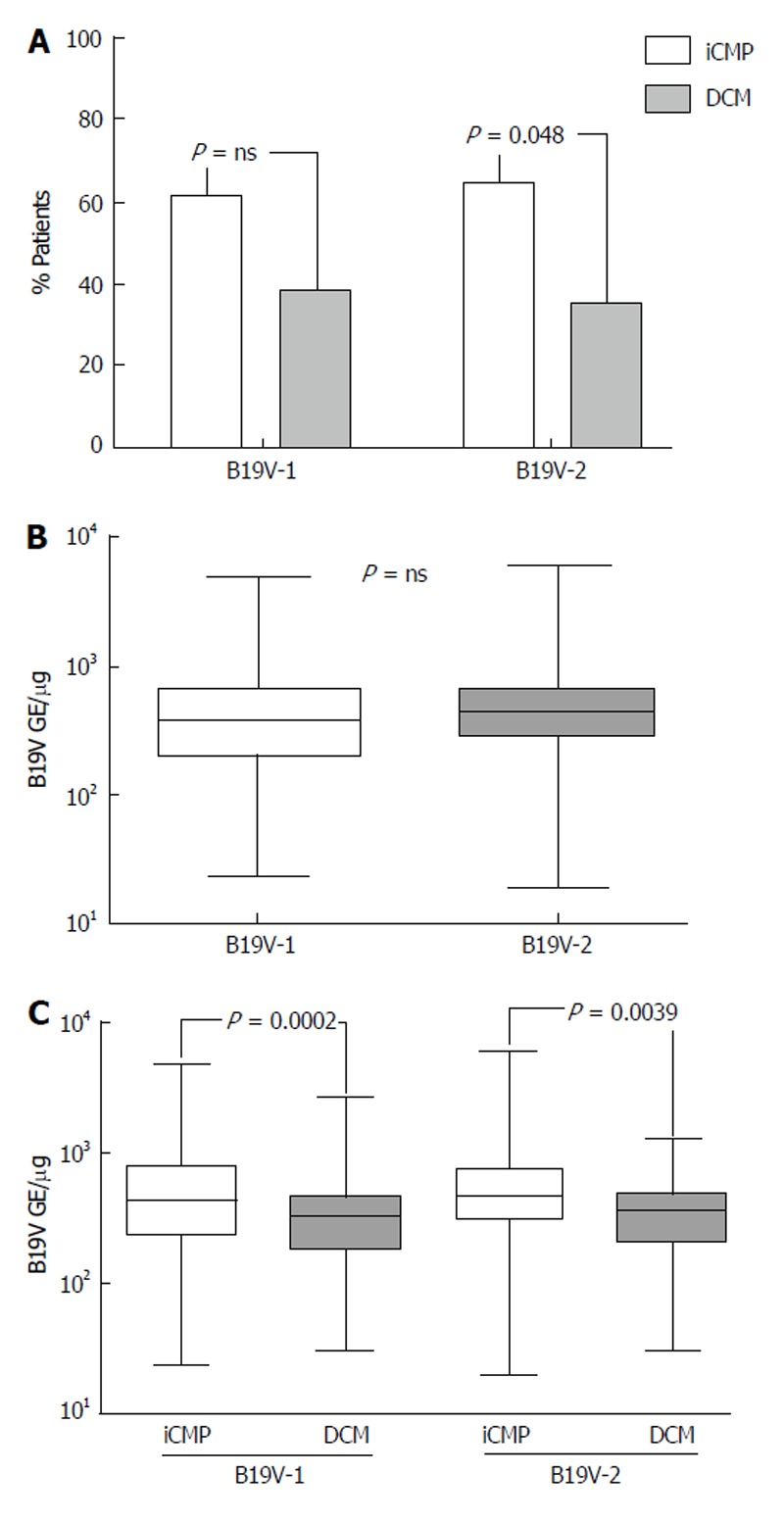
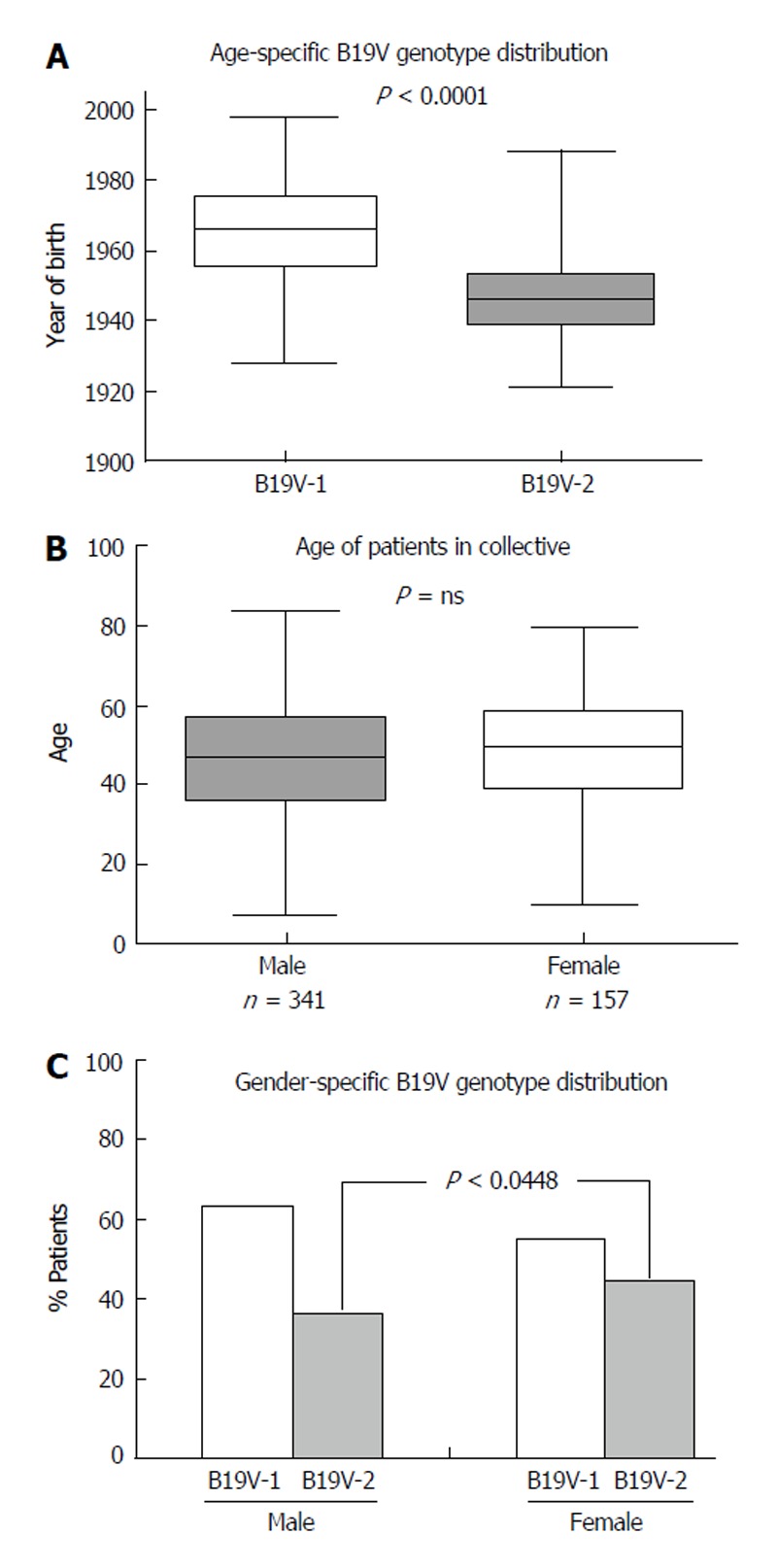
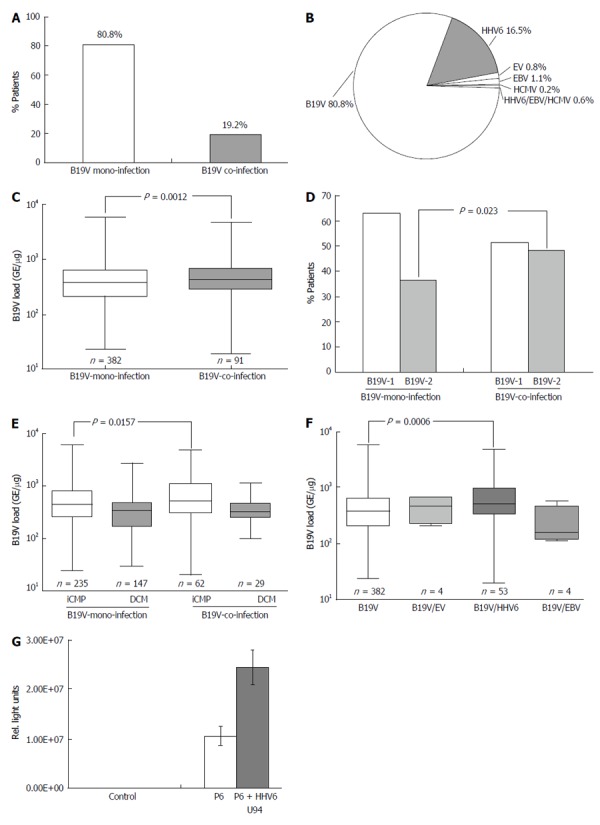
Results: The prevalence of B19V was significantly more likely to be associated with inflammatory cardiomyopathy (iCMP) compared to uninflamed DCM (59.6% vs 35.3%) (P < 0.0001). The detection of B19V-mRNA replication intermediates proved that replication of B19V was present. RFLP-PCR assays showed that B19V-genotype 1 (57.4%) and B19V-genotype 2 (36.7%) were the most prevalent viral genotypes. B19V-genotype 2 was observed more frequently in EMBs with iCMP (65.0%) compared to DCM (35%) (P = 0.049). Although there was no significant difference in gender-specific B19V-loads, women were more frequently infected with B19V-genotype 2 (44.6%) than men (36.0%) (P = 0.0448). Coinfection with B19V and other cardiotropic viruses was found in 19.2% of tissue samples and was associated with higher B19V viral load compared to B19V-monoinfected tissue (P = 0.0012). The most frequent coinfecting virus was human herpes virus 6 (HHV6, 16.5%). B19V-coinfection with HHV6 showed higher B19V-loads compared to B19V-monoinfected EMBs (P = 0.0033), suggesting that HHV6 had transactivated B19V. In vitro experiments confirmed a 2.4-fold increased B19V P6-promoter activity by the HHV6 U94-transactivator.
Conclusion: The finding of significantly increased B19V loads in patients with histologically proven cardiac inflammation suggests a crucial role of B19V-genotypes and reactivation of B19V-infection by HHV6-coinfection in B19V-associated iCMP. Our findings suggest that B19V-infection of the human heart can be a causative event for the development of an endothelial cell-mediated inflammatory disease and that this is related to both viral load and genotype.
Keywords: B19V co-infection; B19V-genotypes; Dilated cardiomyopathy; Myocarditis; Parvovirus B19.
Figures
Similar articles
-
Parvovirus B19 profiles in patients presenting with acute myocarditis and chronic dilated cardiomyopathy.Med Sci Monit. 2008 Dec;14(12):CR589-97. Med Sci Monit. 2008. PMID: 19043365
-
Adaptive immune responses against parvovirus B19 in patients with myocardial disease.J Clin Virol. 2009 Jan;44(1):27-32. doi: 10.1016/j.jcv.2008.09.007. Epub 2008 Nov 5. J Clin Virol. 2009. PMID: 18980860
-
Prevalence of parvovirus B19 and human bocavirus DNA in the heart of patients with no evidence of dilated cardiomyopathy or myocarditis.Clin Infect Dis. 2009 Dec 1;49(11):1660-6. doi: 10.1086/648074. Clin Infect Dis. 2009. PMID: 19863443
-
Systematic Review of PCR Proof of Parvovirus B19 Genomes in Endomyocardial Biopsies of Patients Presenting with Myocarditis or Dilated Cardiomyopathy.Viruses. 2019 Jun 18;11(6):566. doi: 10.3390/v11060566. Viruses. 2019. PMID: 31216741 Free PMC article.
-
Relevance of cardiac parvovirus B19 in myocarditis and dilated cardiomyopathy: review of the literature.Eur J Heart Fail. 2016 Dec;18(12):1430-1441. doi: 10.1002/ejhf.665. Epub 2016 Oct 17. Eur J Heart Fail. 2016. PMID: 27748022 Review.
Cited by
-
Lymphocytic Myocarditis in Children with Parvovirus B19 Infection: Pathological and Molecular Insights.Biomedicines. 2024 Aug 20;12(8):1909. doi: 10.3390/biomedicines12081909. Biomedicines. 2024. PMID: 39200373 Free PMC article.
-
Triggers of Inflammatory Heart Disease.Front Cell Dev Biol. 2020 Mar 24;8:192. doi: 10.3389/fcell.2020.00192. eCollection 2020. Front Cell Dev Biol. 2020. PMID: 32266270 Free PMC article. Review.
-
Myocarditis and inflammatory cardiomyopathy: current evidence and future directions.Nat Rev Cardiol. 2021 Mar;18(3):169-193. doi: 10.1038/s41569-020-00435-x. Epub 2020 Oct 12. Nat Rev Cardiol. 2021. PMID: 33046850 Free PMC article. Review.
-
Existence of various human parvovirus B19 genotypes in Chinese plasma pools: genotype 1, genotype 3, putative intergenotypic recombinant variants and new genotypes.Virol J. 2016 Sep 17;13(1):155. doi: 10.1186/s12985-016-0611-6. Virol J. 2016. PMID: 27639978 Free PMC article.
-
Clinical impact & pathogenic mechanisms of human parvovirus B19: A multiorgan disease inflictor incognito.Indian J Med Res. 2018 Oct;148(4):373-384. doi: 10.4103/ijmr.IJMR_533_18. Indian J Med Res. 2018. PMID: 30666000 Free PMC article.
References
-
- Bültmann BD, Klingel K, Sotlar K, Bock CT, Baba HA, Sauter M, Kandolf R. Fatal parvovirus B19-associated myocarditis clinically mimicking ischemic heart disease: an endothelial cell-mediated disease. Hum Pathol. 2003;34:92–95. - PubMed
-
- Klingel K, Sauter M, Bock CT, Szalay G, Schnorr JJ, Kandolf R. Molecular pathology of inflammatory cardiomyopathy. Med Microbiol Immunol. 2004;193:101–107. - PubMed
-
- Mahfoud F, Gärtner B, Kindermann M, Ukena C, Gadomski K, Klingel K, Kandolf R, Böhm M, Kindermann I. Virus serology in patients with suspected myocarditis: utility or futility? Eur Heart J. 2011;32:897–903. - PubMed
-
- Bock CT, Klingel K, Kandolf R. Human parvovirus B19-associated myocarditis. N Engl J Med. 2010;362:1248–1249. - PubMed
-
- Ruppert V, Meyer T, Balbach A, Richter A, Müller HH, Maisch B, Pankuweit S. Genotype-specific effects on left ventricular function in parvovirus B19-positive patients with dilated cardiomyopathy. J Med Virol. 2011;83:1818–1825. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
