

Coronary artery disease in congenital single coronary artery in adults: A Dutch case series
- PMID: 24772259
- PMCID: PMC3999339
- DOI: 10.4330/wjc.v6.i4.196
Coronary artery disease in congenital single coronary artery in adults: A Dutch case series
Abstract
Aim: To assess the current diagnostic and therapeutic management and the clinical implications of congenital single coronary artery (SCA) in adults.
Methods: We identified 15 patients with a SCA detected from four Dutch angiography centers in the period between 2010 and 2013. Symptomatic patients who underwent routine diagnostic coronary angiography (CAG) for suspected coronary artery disease and who incidentally were found to have isolated SCA were analyzed.
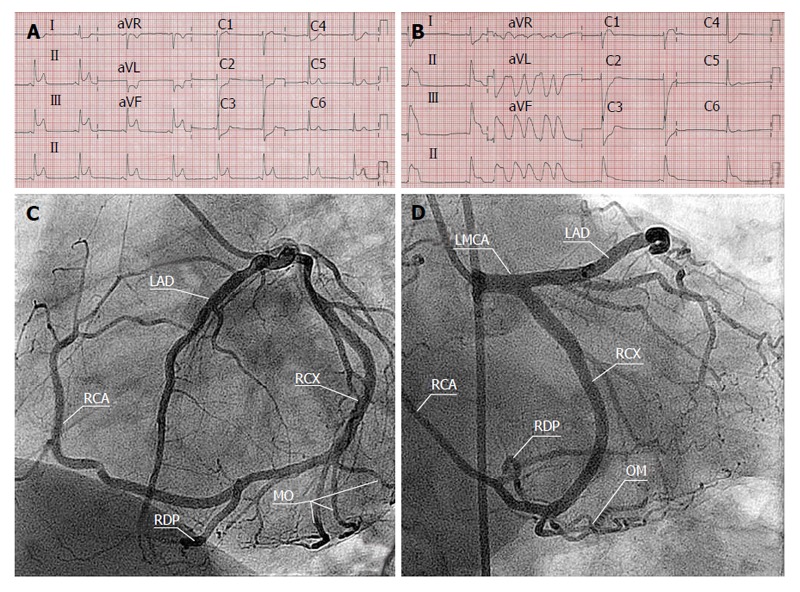
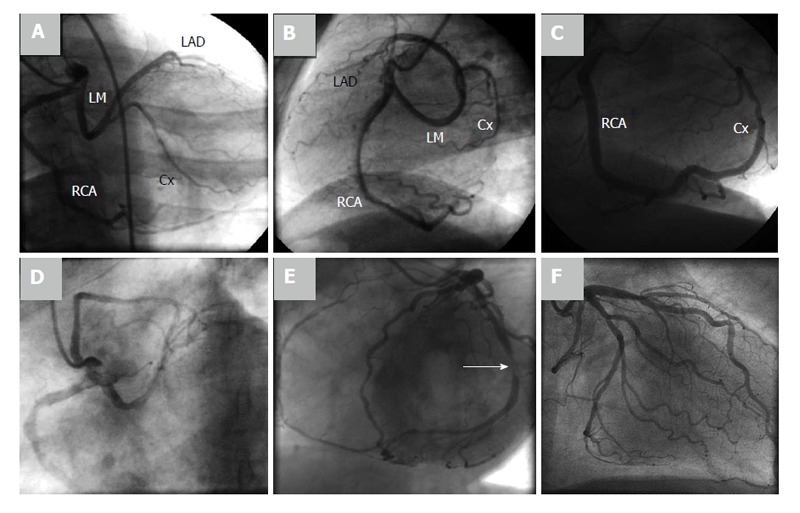
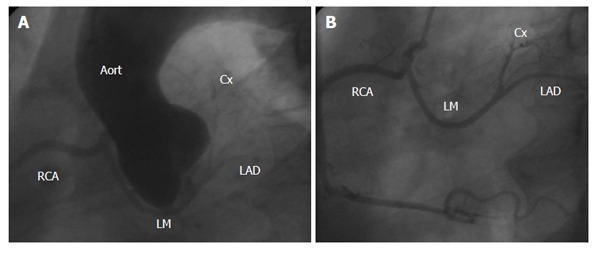
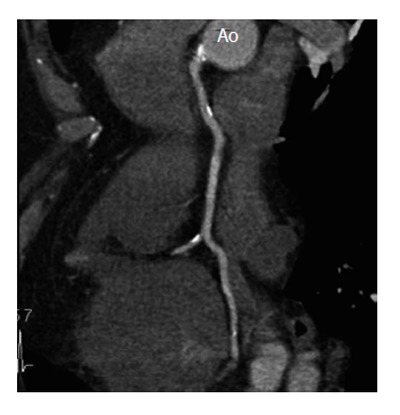
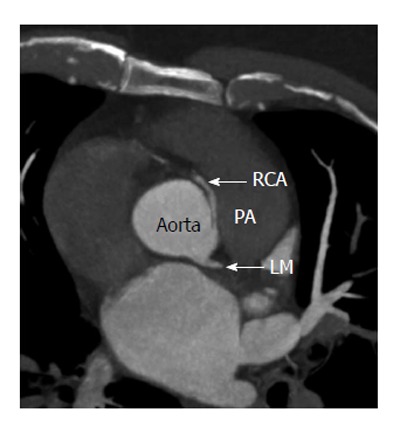
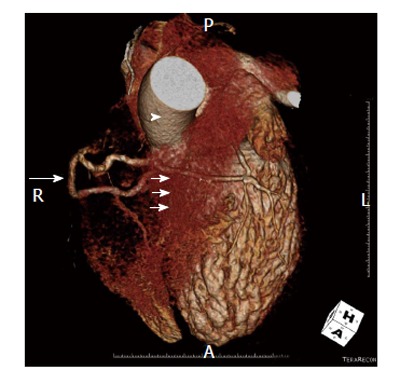
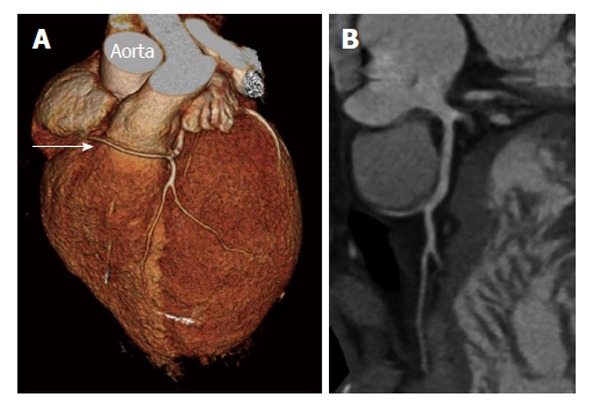
Results: Fifteen (7 females) with a mean age of 58.5 ± 13.78 years (range 43-86) had a SCA. Conventional CAG demonstrated congenital isolated SCA originating as a single ostium from the right sinus of Valsalva in 6 patients and originating from the left in 9 patients. Minimal to moderate coronary atherosclerotic changes were found in 4, and severe stenotic lesions in another 4 patients. Seven patients were free of coronary atherosclerosis. Runs of non-sustained ventricular tachycardia were documented in 2 patients, one of whom demonstrated transmural ischemic changes on presentation. Myocardial perfusion scintigraphic evidence of transmural myocardial ischemia was found in 1 patient due to kinking and squeezing of the SCA with an interarterial course between the aorta and pulmonary artery. Multi-slice computed tomography (MSCT) was helpful to delineate the course of the anomalous artery relative to the aorta and pulmonary artery. Percutaneous coronary intervention was successfully performed in 3 patients. Eight patients were managed medically. Arterial bypass graft was performed in 4 patients with the squeezed SCA.
Conclusion: SCA may be associated with transient transmural myocardial ischemia and aborted sudden death in the absence of coronary atherosclerosis. The availability and sophistication of MSCT facilitates the delineation of the course of a SCA. We present a Dutch case series and review of the literature.
Keywords: Congenital heart disease; Coronary angiography; Coronary artery anomaly; Coronary artery disease; Multi-slice computed tomography; Single coronary artery.
Figures
Similar articles
-
Anomalous origin of coronary artery from the opposite aortic sinus of Valsalva-a single center experience with a therapeutic conundrum.Indian Heart J. 2021 May-Jun;73(3):289-294. doi: 10.1016/j.ihj.2021.03.012. Epub 2021 Apr 3. Indian Heart J. 2021. PMID: 34154744 Free PMC article.
-
Acute coronary syndrome in a patient with a single coronary artery arising from the right sinus of Valsalva.World J Cardiol. 2012 Aug 26;4(8):264-6. doi: 10.4330/wjc.v4.i8.264. World J Cardiol. 2012. PMID: 22953025 Free PMC article.
-
Right single coronary artery as an incidental finding in Takotsubo syndrome and acute heart failure: Case report and review of the literature.Rev Port Cardiol (Engl Ed). 2019 Mar;38(3):215-223. doi: 10.1016/j.repc.2018.06.013. Epub 2019 Apr 20. Rev Port Cardiol (Engl Ed). 2019. PMID: 31014998 Review. English, Portuguese.
-
A Rare Case of Single Coronary Artery with Atherosclerotic Lesions Arising from the Right Sinus of Valsalva.N Am J Med Sci. 2016 Feb;8(2):114-6. doi: 10.4103/1947-2714.177345. N Am J Med Sci. 2016. PMID: 27042610 Free PMC article.
-
Acquired and congenital coronary artery abnormalities.Cardiol Young. 2017 Jan;27(S1):S31-S35. doi: 10.1017/S1047951116002201. Cardiol Young. 2017. PMID: 28084958 Review.
Cited by
-
A Rare Anatomical Variant: Congenital Absence of the Right Coronary Artery with Left Circumflex Artery Supplying the Right Coronary Artery (RCA) Territory.Am J Case Rep. 2021 Aug 26;22:e932248. doi: 10.12659/AJCR.932248. Am J Case Rep. 2021. PMID: 34437516 Free PMC article.
-
A rare case of single right coronary artery arising from the right sinus of Valsalva with severe three-vessel disease.J Geriatr Cardiol. 2017 Mar;14(3):218-221. doi: 10.11909/j.issn.1671-5411.2017.03.003. J Geriatr Cardiol. 2017. PMID: 28592964 Free PMC article. No abstract available.
-
Prevalence, Spectrum, and Outcomes of Single Coronary Artery Detected on Coronary Computed Tomography Angiography (CCTA).Radiol Res Pract. 2019 Aug 6;2019:2940148. doi: 10.1155/2019/2940148. eCollection 2019. Radiol Res Pract. 2019. PMID: 31467712 Free PMC article.
-
Complex single ostium coronary artery from the right coronary sinus with unique course of anomalous left circumflex coronary artery.J Cardiol Cases. 2015 Nov 23;13(2):56-59. doi: 10.1016/j.jccase.2015.10.005. eCollection 2016 Feb. J Cardiol Cases. 2015. PMID: 30524556 Free PMC article.
-
A rare case of single right coronary artery with congenital absence of left coronary artery in an adult: a case report.J Cardiothorac Surg. 2015 Apr 21;10:57. doi: 10.1186/s13019-015-0267-0. J Cardiothorac Surg. 2015. PMID: 25896277 Free PMC article.
References
-
- Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979;130:39–47. - PubMed
-
- Shirani J, Roberts WC. Solitary coronary ostium in the aorta in the absence of other major congenital cardiovascular anomalies. J Am Coll Cardiol. 1993;21:137–143. - PubMed
-
- Smith JC. Review of single coronary artery with report of 2 cases. Circulation. 1950;1:1168–1175. - PubMed
-
- Halperin IC, Penny JL, Kennedy RJ. Single coronary artery. Antemortem diagnosis in a patient with congestive heart failure. Am J Cardiol. 1967;19:424–427. - PubMed
-
- Desmet W, Vanhaecke J, Vrolix M, Van de Werf F, Piessens J, Willems J, de Geest H. Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies. Eur Heart J. 1992;13:1637–1640. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
