

Door-to-puncture: a practical metric for capturing and enhancing system processes associated with endovascular stroke care, preliminary results from the rapid reperfusion registry
- PMID: 24772523
- PMCID: PMC4187502
- DOI: 10.1161/jaha.114.000859
Door-to-puncture: a practical metric for capturing and enhancing system processes associated with endovascular stroke care, preliminary results from the rapid reperfusion registry
Abstract
Background: In 2011, the Brain Attack Coalition proposed door-to-treatment times of 2 hours as a benchmark for patients undergoing intra-arterial therapy (IAT). We designed the Rapid Reperfusion Registry to capture the percentage of stroke patients who meet the target and its impact on outcomes.
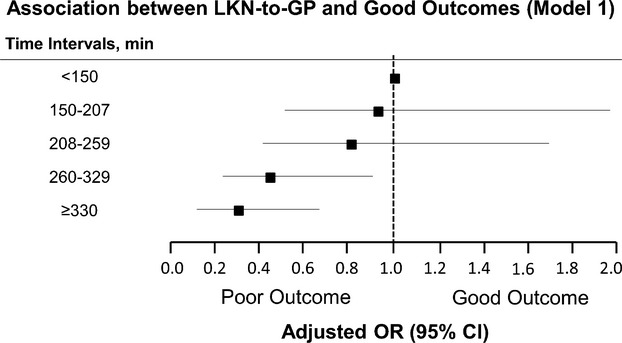
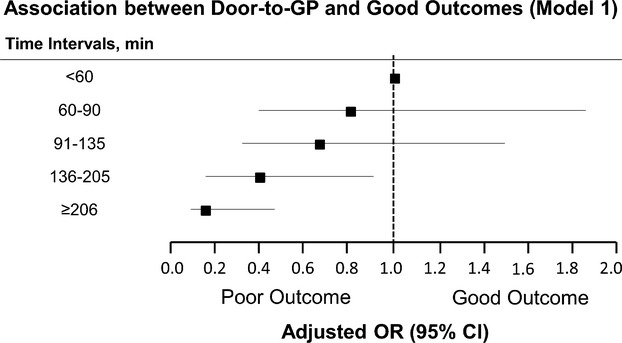
Methods and results: This is a retrospective analysis of anterior circulation patients treated with IAT within 9 hours of symptom onset. Data was collected from December 31, 2011 to December 31, 2012 at 2 centers and from July 1, 2012 to December 31, 2012 at 7 centers. Short “Door-to-Puncture” (D2P) time was hypothesized to be associated with good patient outcomes. A total of 478 patients with a mean age of 68±14 years and median National Institutes of Health Stroke Scale (NIHSS) of 18 (IQR 14 to 21) were analyzed. The median times for IAT delivery were 234 minutes (IQR 163 to 304) for “last known normal-to-groin puncture” time (LKN-to-GP) and 112 minutes (IQR 68 to 176) for D2P time. The overall good outcome rate was 39.7% for the entire cohort. In a multivariable model adjusting for age, NIHSS, hypertension, diabetes, reperfusion status, and symptomatic hemorrhage, both short LKN-to-GP (OR 0.996; 95% CI [0.993 to 0.998]; P<0.001) and short D2P times (OR 0.993, 95% CI [0.990 to 0.996]; P<0.001) were associated with good outcomes. Only 52% of all patients in the registry achieved the targeted D2P time of 2 hours.
Conclusions: The time interval of D2P presents a clinically relevant time frame by which system processes can be targeted to streamline the delivery of IAT care nationally. At present, there is much opportunity to enhance outcomes through reducing D2P.
Figures
References
-
- Brindis RG, Fitzgerald S, Anderson HV, Shaw RE, Weintraub WS, Williams JF. The American College of Cardiology‐National Cardiovascular Data Registry (ACC‐NCDR): building a national clinical data repository. J Am Coll Cardiol. 2001; 37:2240-2245 - PubMed
-
- Moussa I, Hermann A, Messenger JC, Dehmer GJ, Weaver WD, Rumsfeld JS, Masoudi FA. The NCDR CathPCI Registry: a US national perspective on care and outcomes for percutaneous coronary intervention. Heart. 2013; 99:297-303 - PubMed
-
- Bradley EH, Nallamothu BK, Herrin J, Ting HH, Stern AF, Nembhard IM, Yuan CT, Green JC, Kline‐Rogers E, Wang Y, Curtis JP, Webster TR, Masoudi FA, Fonarow GC, Brush JE, Jr, Krumholz HM. National efforts to improve door‐to‐balloon time results from the Door‐to‐Balloon Alliance. J Am Coll Cardiol. 2009; 54:2423-2429 - PubMed
-
- Gupta R, Horev A, Nguyen T, Gandhi D, Wisco D, Glenn BA, Tayal AH, Ludwig B, Terry JB, Gershon RY, Jovin T, Clemmons PF, Frankel MR, Cronin CA, Anderson AM, Hussain MS, Sheth KN, Belagaje SR, Tian M, Nogueira RG. Higher volume endovascular stroke centers have faster times to treatment, higher reperfusion rates and higher rates of good clinical outcomes. J Neurointerv Surg. 2013; 5:294-297 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
