

Biomechanics of corneal ectasia and biomechanical treatments
- PMID: 24774009
- PMCID: PMC4850839
- DOI: 10.1016/j.jcrs.2014.04.013
Biomechanics of corneal ectasia and biomechanical treatments
Abstract
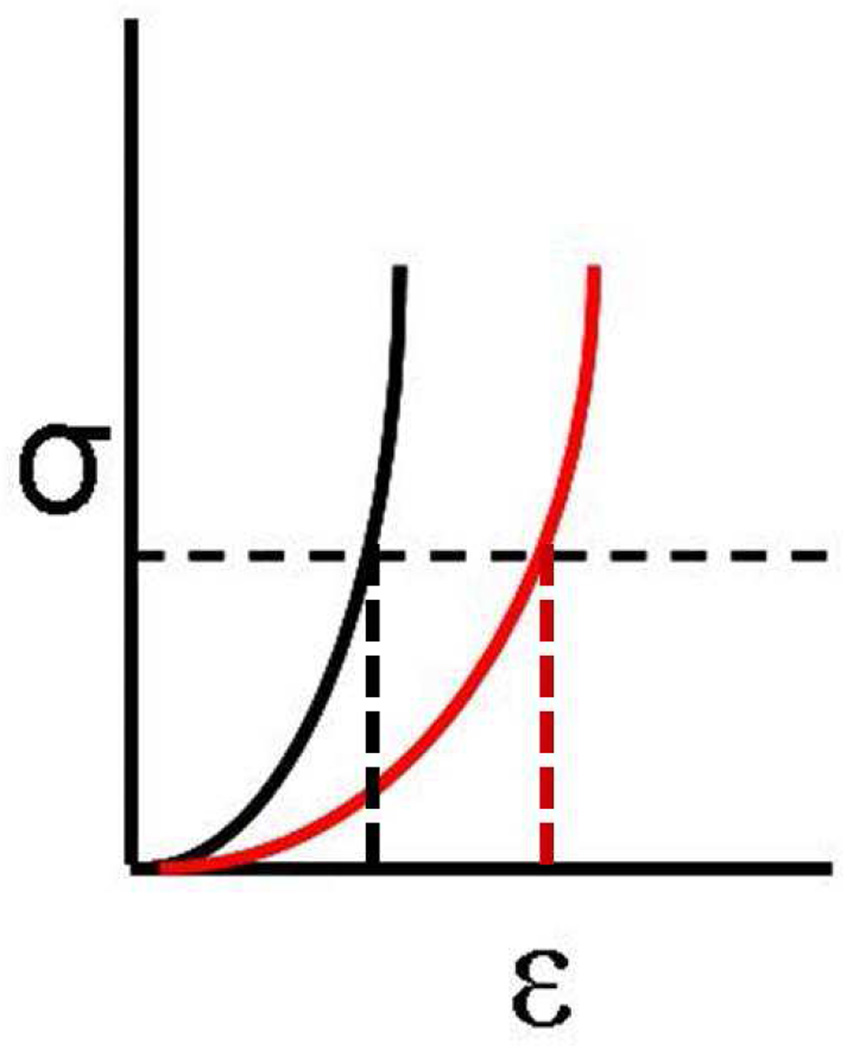
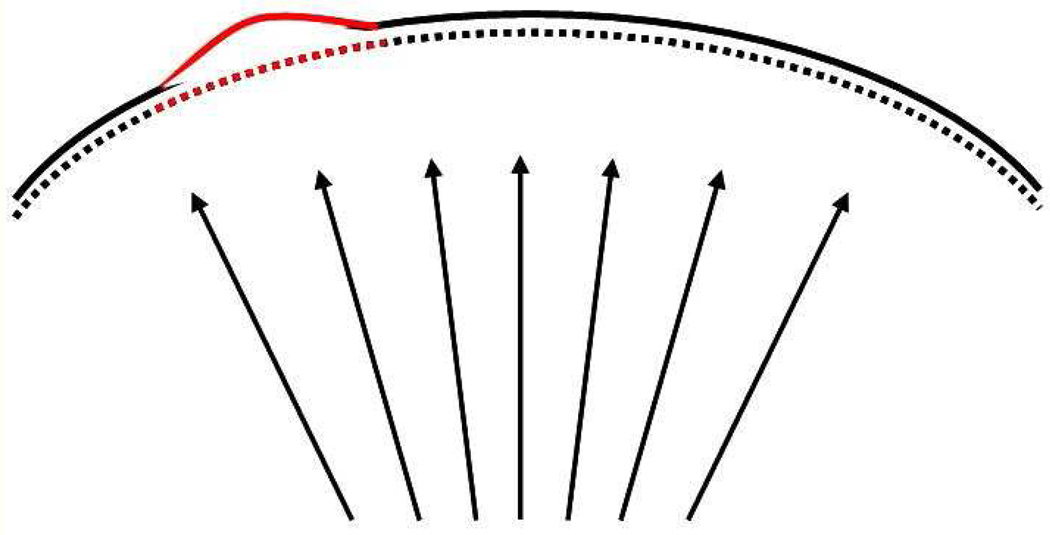
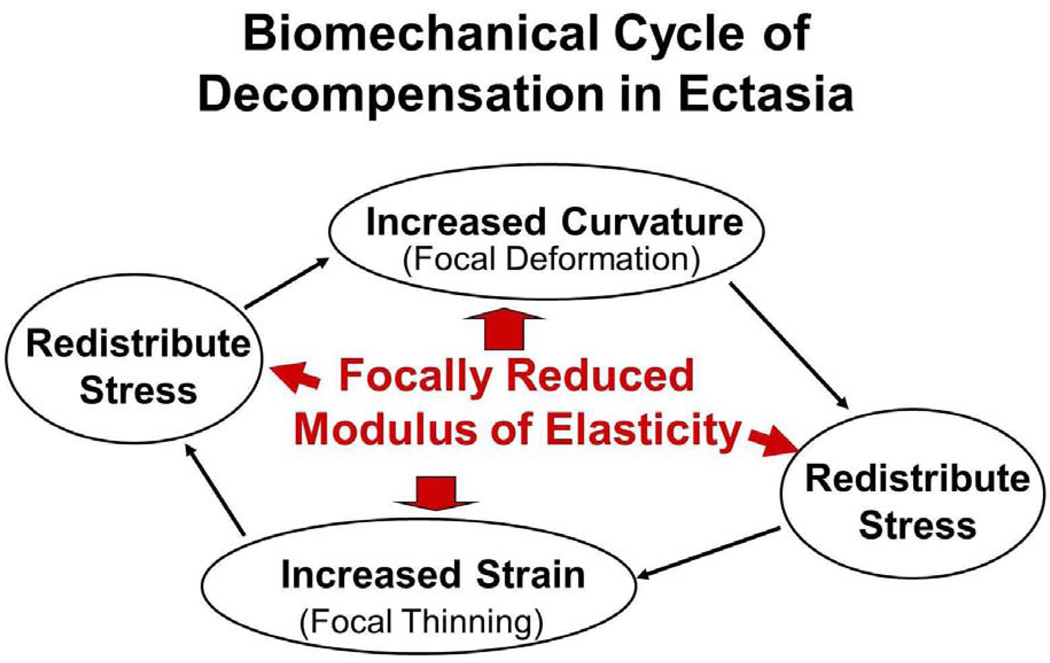
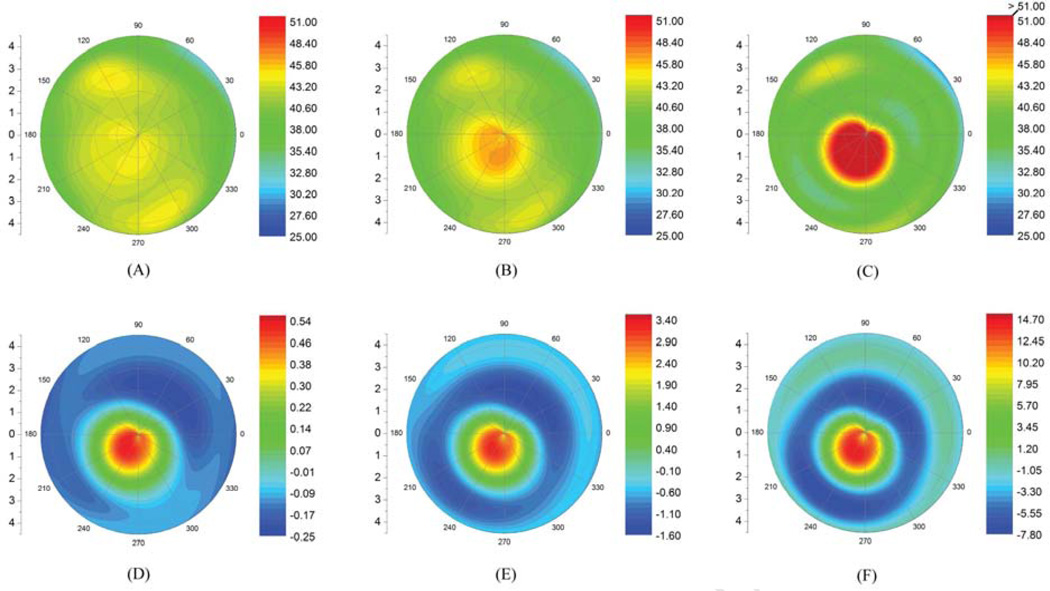
Many algorithms exist for the topographic/tomographic detection of corneas at risk for post-refractive surgery ectasia. It is proposed that the reason for the difficulty in finding a universal screening tool based on corneal morphologic features is that curvature, elevation, and pachymetric changes are all secondary signs of keratoconus and post-refractive surgery ectasia and that the primary abnormality is in the biomechanical properties. It is further proposed that the biomechanical modification is focal in nature, rather than a uniform generalized weakening, and that the focal reduction in elastic modulus precipitates a cycle of biomechanical decompensation that is driven by asymmetry in the biomechanical properties. This initiates a repeating cycle of increased strain, stress redistribution, and subsequent focal steepening and thinning. Various interventions are described in terms of how this cycle of biomechanical decompensation is interrupted, such as intrastromal corneal ring segments, which redistribute the corneal stress, and collagen crosslinking, which modifies the basic structural properties.
Financial disclosures: Proprietary or commercial disclosures are listed after the references.
Copyright © 2014 ASCRS and ESCRS. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Kim W-J, Rabinowitz YS, Meisler DM, Wilson SE. Keratocyte apoptosis associated with keratoconus. Exp Eye Res. 1999;69:475–481. - PubMed
-
- Matthews FJ, Cook SD, Majid MA, Dick AD, Smith VA. Changes in the balance of the tissue inhibitor of matrix metalloproteinases (TIMPs)-1 and -3 may promote keratocyte apoptosis in keratoconus. Exp Eye Res. 2007;84:1125–1134. - PubMed
-
- Meek KM, Tuft SJ, Huang Y, Gill PS, Hayes S, Newton RH, Bron AJ. Changes in collagen orientation and distribution in keratoconus corneas. [Accessed January 25, 2014];Invest Ophthalmol Vis Sci. 2005 46:1948–1956. Available at: http://www.iovs.org/content/46/6/1948.full.pdf. - PubMed
-
- Morishige N, Wahlert AJ, Kenney MC, Brown DJ, Kawamoto K, Chikama T-i, Nishida T, Jester JV. Second-harmonic imaging microscopy of normal human and keratoconus cornea. [Accessed January 25, 2014];Invest Ophthalmol Vis Sci. 2007 48:1087–1094. Available at: http://www.iovs.org/cgi/reprint/48/3/1087. - PMC - PubMed
-
- Foster CS, Yamamoto GK. Ocular rigidity in keratoconus. Am J Ophthalmol. 1978;86:802–806. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
