

Relationship between ICU bed availability, ICU readmission, and cardiac arrest in the general wards
- PMID: 24776607
- PMCID: PMC4134732
- DOI: 10.1097/CCM.0000000000000401
Relationship between ICU bed availability, ICU readmission, and cardiac arrest in the general wards
Abstract
Objective: The decision to admit a patient to the ICU is complex, reflecting patient factors and available resources. Previous work has shown that ICU census does not impact mortality of patients admitted to the ICU. However, the effect of ICU bed availability on patients outside the ICU is unknown. We sought to determine the association between ICU bed availability, ICU readmissions, and ward cardiac arrests.
Design: In this observational study using data collected between 2009 and 2011, rates of ICU readmission and ward cardiac arrest were determined per 12-hour shift. The relationship between these rates and the number of available ICU beds at the start of each shift (accounting for census and nursing capacity) was investigated. Grouped logistic regression was used to adjust for potential confounders.
Setting: Five specialized adult ICUs comprising 63 adult ICU beds in an academic medical center.
Patients: Any patient admitted to a non-ICU inpatient unit was counted in the ward census and considered at risk for ward cardiac arrest. Patients discharged from an ICU were considered at risk for ICU readmission.
Interventions: None.
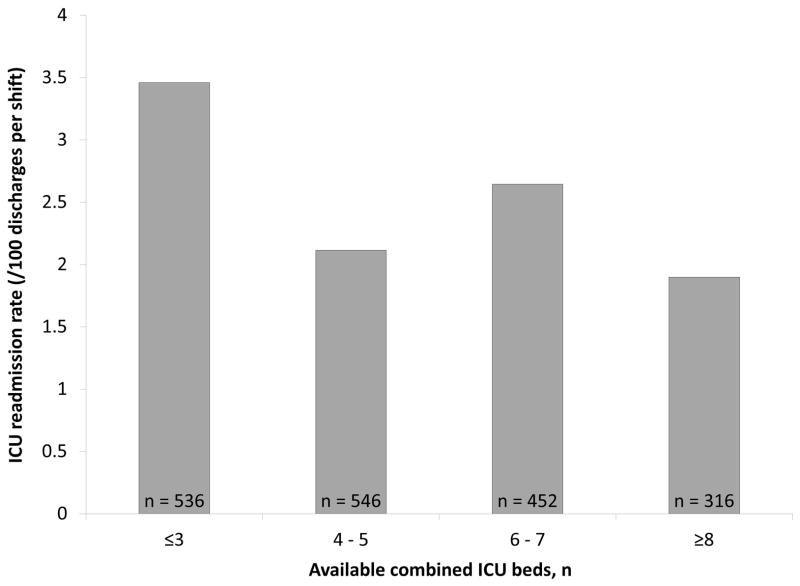
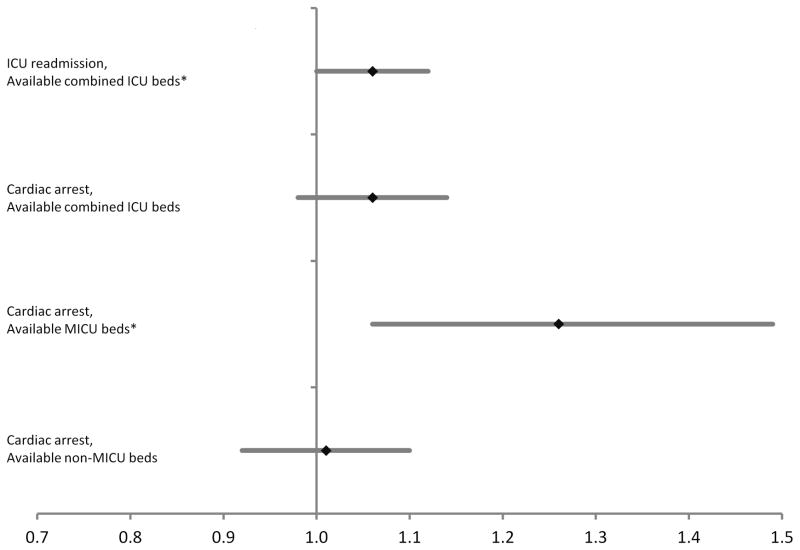
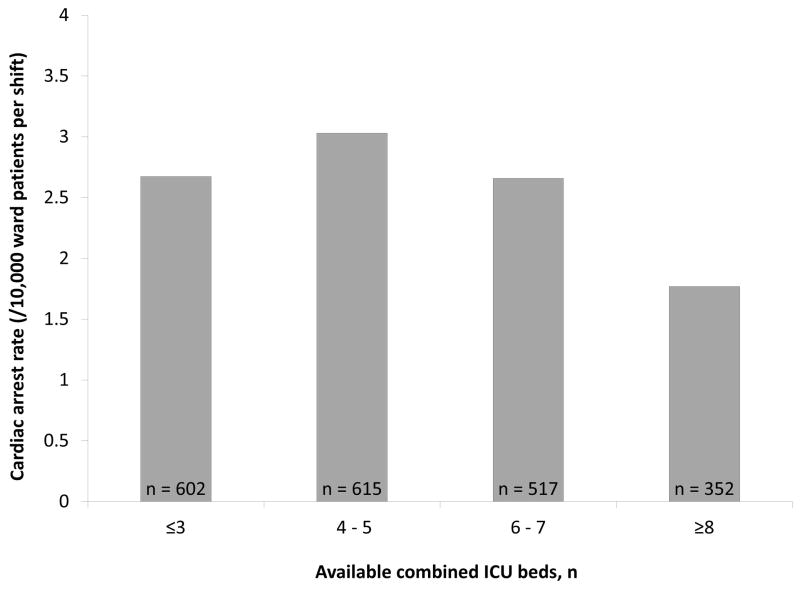
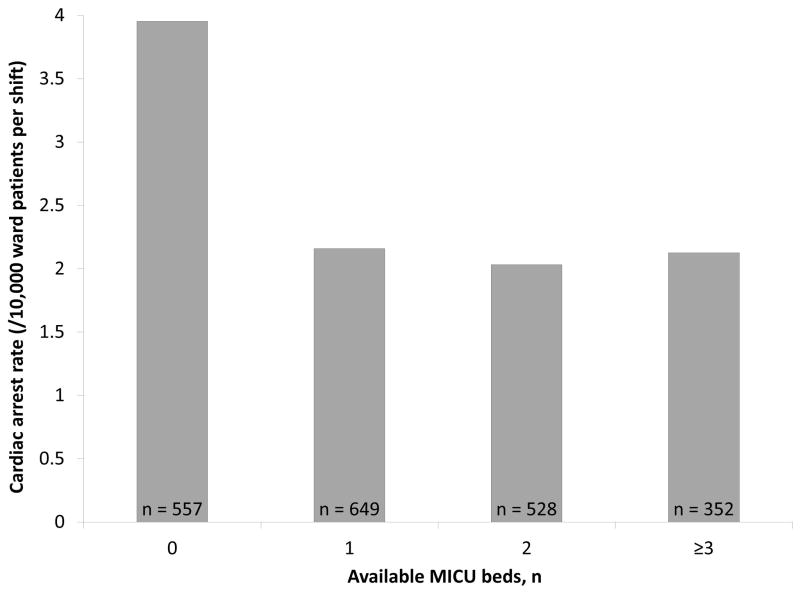
Measurements and main results: Data were available for 2,086 of 2,190 shifts. The odds of ICU readmission increased with each decrease in the overall number of available ICU beds (odds ratio = 1.06; 95% CI, 1.00-1.12; p = 0.03), with a similar but not statistically significant association demonstrated in ward cardiac arrest rate (odds ratio = 1.06; 95% CI, 0.98-1.14; p = 0.16). In subgroup analysis, the odds of ward cardiac arrest increased with each decrease in the number of medical ICU beds available (odds ratio = 1.26; 95% CI, 1.06-1.49; p = 0.01).
Conclusions: Reduced ICU bed availability is associated with increased rates of ICU readmission and ward cardiac arrest. This suggests that systemic factors are associated with patient outcomes, and flexible critical care resources may be needed when demand is high.
Figures
References
-
- Halpern NA, Pastores SM. Critical care medicine in the united states 2000–2005: An analysis of bed numbers, occupancy rates, payer mix, and costs. Crit Care Med. 2010;38:65–71. - PubMed
-
- Needham DM, Bronskill SE, Calinawan JR, et al. Projected incidence of mechanical ventilation in ontario to 2026: Preparing for the aging baby boomers. Crit Care Med. 2005;33:574–579. - PubMed
-
- Strauss MJ, LoGerfo JP, Yeltatzie JA, et al. Rationing of intensive care unit services. JAMA. 1986;255:1143–1146. - PubMed
-
- Singer DE, Mulley AG, Thibault GE. Rationing intensive care - physician responses to a resource shortage. NEJM. 1983;309:1155–1160. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
