

Dipstick screening for urinary tract infection in febrile infants
- PMID: 24777232
- PMCID: PMC4006440
- DOI: 10.1542/peds.2013-3291
Dipstick screening for urinary tract infection in febrile infants
Abstract
Objective: This study compares the performance of urine dipstick alone with urine microscopy and with both tests combined as a screen for urinary tract infection (UTI) in febrile infants aged 1 to 90 days.
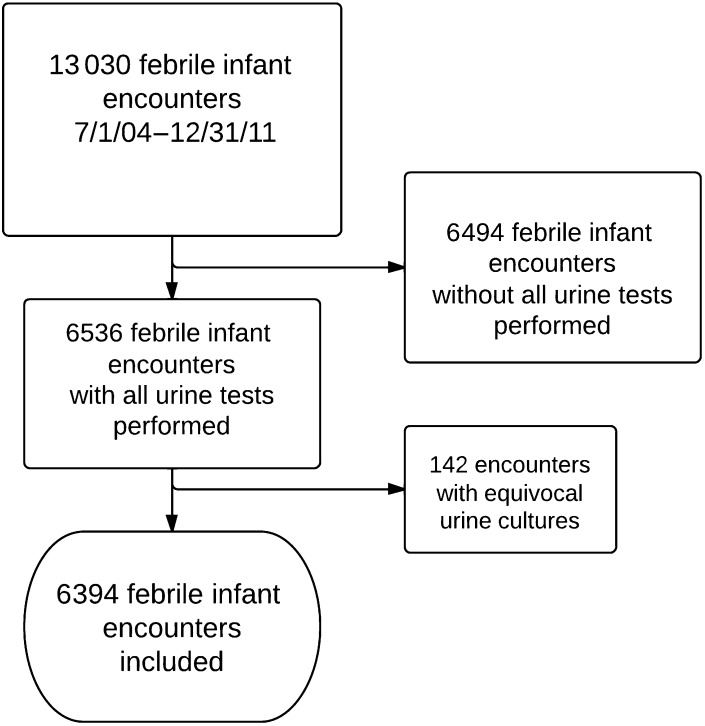
Methods: We queried the Intermountain Healthcare data warehouse to identify febrile infants with urine dipstick, microscopy, and culture performed between 2004 and 2011. UTI was defined as >50 000 colony-forming units per milliliter of a urinary pathogen. We compared the performance of urine dipstick with unstained microscopy or both tests combined ("combined urinalysis") to identify UTI in infants aged 1 to 90 days.
Results: Of 13 030 febrile infants identified, 6394 (49%) had all tests performed and were included in the analysis. Of these, 770 (12%) had UTI. Urine culture results were positive within 24 hours in 83% of UTIs. The negative predictive value (NPV) was >98% for all tests. The combined urinalysis NPV was 99.2% (95% confidence interval: 99.1%-99.3%) and was significantly greater than the dipstick NPV of 98.7% (98.6%-98.8%). The dipstick positive predictive value was significantly greater than combined urinalysis (66.8% [66.2%-67.4%] vs 51.2% [50.6%-51.8%]). These data suggest 8 febrile infants would be predicted to have a false-positive combined urinalysis for every 1 infant with UTI initially missed by dipstick screening.
Conclusions: Urine dipstick testing compares favorably with both microscopy and combined urinalysis in febrile infants aged 1 to 90 days. The urine dipstick test may be an adequate stand-alone screen for UTI in febrile infants while awaiting urine culture results.
Keywords: infant; leukocyte esterase; newborn; nitrites; predictive value of tests; reagent strips; urinalysis; urinary tract infection; utilization.
Copyright © 2014 by the American Academy of Pediatrics.
Figures
References
-
- Byington CL, Enriquez FR, Hoff C, et al. . Serious bacterial infections in febrile infants 1 to 90 days old with and without viral infections. Pediatrics. 2004;113(6):1662–1666 - PubMed
-
- Baraff LJ, Oslund SA, Schriger DL, Stephen ML. Probability of bacterial infections in febrile infants less than three months of age: a meta-analysis. Pediatr Infect Dis J. 1992;11(4):257–264 - PubMed
-
- Byington CL, Reynolds CC, Korgenski K, et al. . Costs and infant outcomes after implementation of a care process model for febrile infants. Pediatrics. 2012;130(1). Available at: www.pediatrics.org/cgi/content/full/130/1/e16 - PMC - PubMed
-
- Dagan R, Powell KR, Hall CB, Menegus MA. Identification of infants unlikely to have serious bacterial infection although hospitalized for suspected sepsis. J Pediatr. 1985;107(6):855–860 - PubMed
-
- Zorc JJ, Levine DA, Platt SL, et al. Multicenter RSV-SBI Study Group of the Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics . Clinical and demographic factors associated with urinary tract infection in young febrile infants. Pediatrics. 2005;116(3):644–648 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
