

Ilizarov fixator combined with an intramedullary nail for tibial nonunions with bone loss: is it effective?
- PMID: 24777722
- PMCID: PMC4397756
- DOI: 10.1007/s11999-014-3640-8
Ilizarov fixator combined with an intramedullary nail for tibial nonunions with bone loss: is it effective?
Abstract
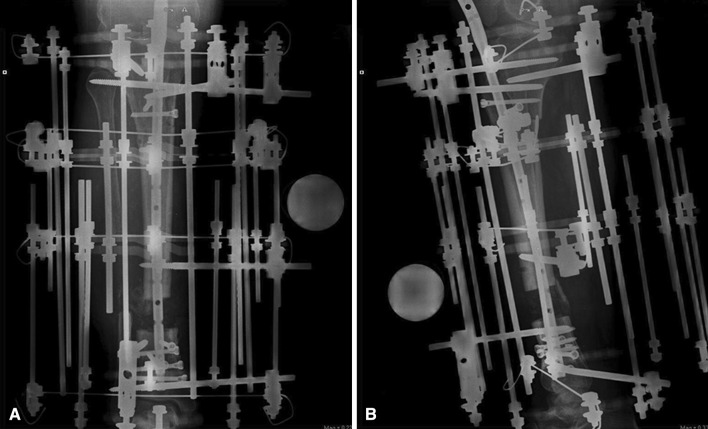
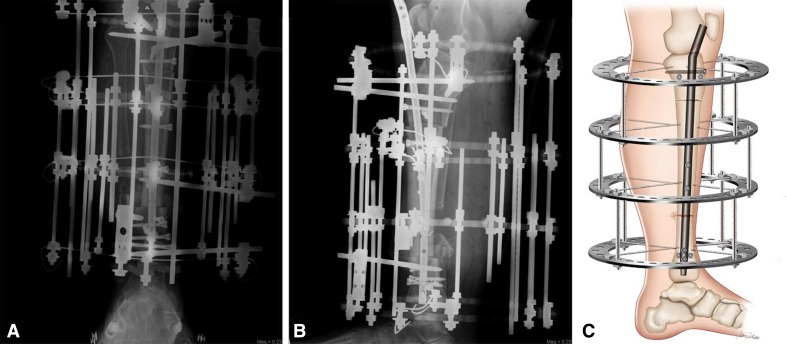
Background: Treatment of tibial nonunion with bone loss is extremely difficult. A variety of techniques have been described, but each has shortcomings, in particular prolonged external fixation time as well as serious complications such as nonunion and infection. Accordingly, we developed a technique that seeks to reduce these complications by using a circular external fixator in addition to an intramedullary nail to achieve union, limb lengthening, and stability of the regenerated segment.
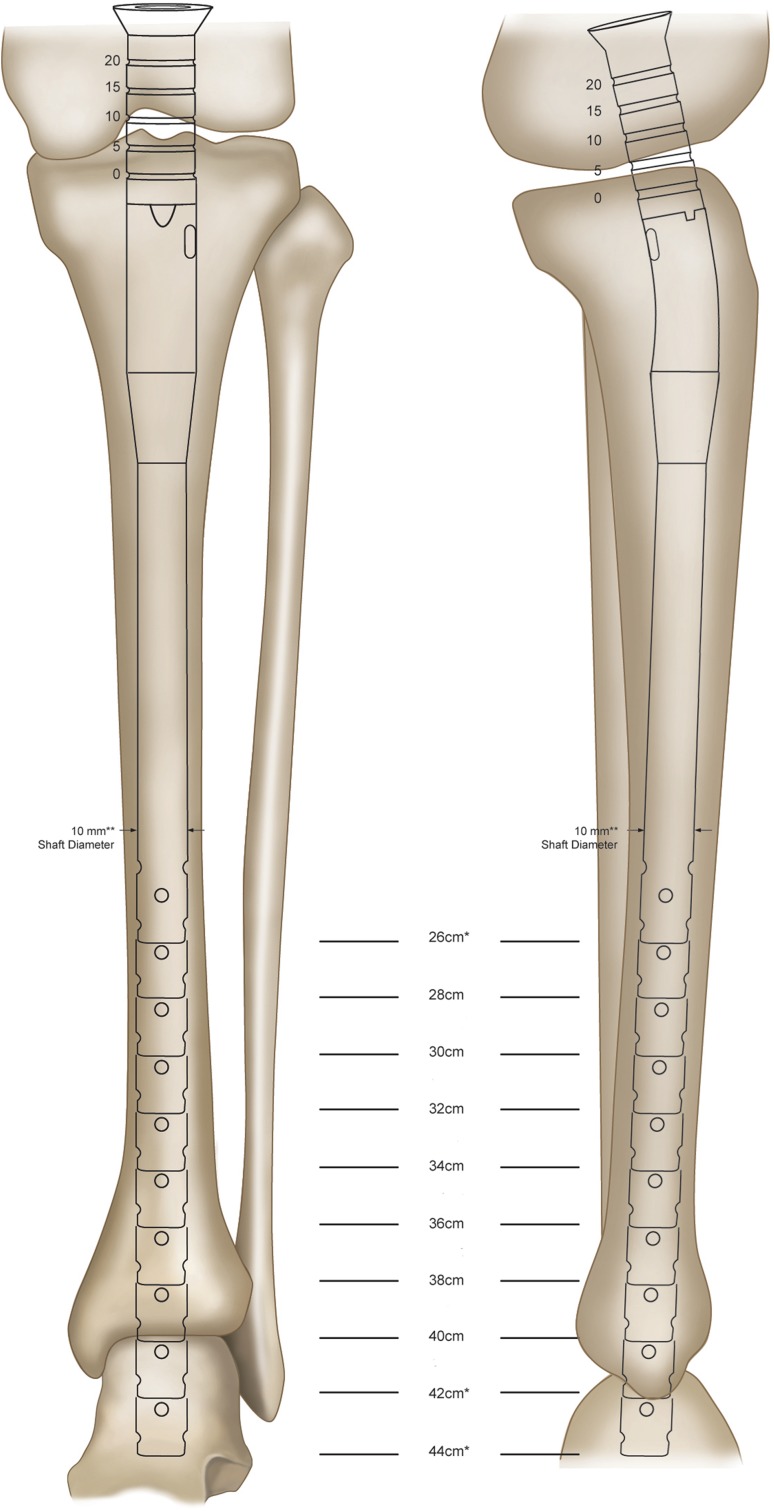
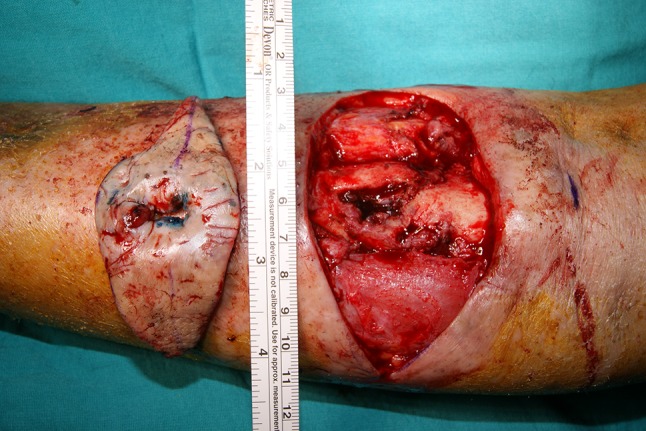
Description of technique: First, the pseudoarthrosis area is resected, and acute compression is continued until bone contact at the docking site was achieved. Then primary grafting is applied to the docking site using a graft harvested from the patient's iliac bone, and the predrilled nail holes localized on the middle segment of the tibia are locked with a free-hand technique. Finally, lengthening is performed to overcome the leg-length discrepancy with an external fixator.
Methods: Between 2008 and 2011, this technique was used to treat five patients with tibial nonunion with bone loss. All patients were available for a minimum of a 14-month followup (mean, 30 months; range, 14-58 months). General indications for the procedure were age older than 16 years, tibial nonunion with bone loss, and the absence of any psychiatric disorder. We evaluated external fixation time, external fixation index (defined as the duration of external fixation in months divided by the total amount of bone transported and/or the amount of lengthening in centimeters), and time to union on plain radiographs, clinical results using the Paley bone and functional assessment scores, and postoperative complications from chart review.
Results: The external fixation time was 4 months (range, 3-5 months), and the average external fixation index was 0.4 months/cm. The mean time to bone union was 4.6 months (range, 3.5-5.5 months). All angles were determined to be in the normal range. No patients developed refracture or malalignment either on the docking site or the osteotomy site. Paley bone evaluation results were excellent in all five patients, and Paley functional results were excellent in four and good in one. We observed 10 pin-site infections as minor complications, and one patient was left with a residual equinus deformity of 5° as a major complication according to the Paley classification.
Conclusions: Our technique combining acute shortening and distraction osteogenesis had promising results for the treatment of tibial nonunion with bone loss in a small group of patients. However, future studies directly comparing available approaches to this difficult problem are required. Because this problem is uncommon, these studies will almost certainly require the cooperation of multiple large participating centers.
Level of evidence: Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures



Similar articles
-
Bifocal compression-distraction in the acute treatment of grade III open tibia fractures with bone and soft-tissue loss: a report of 24 cases.J Orthop Trauma. 2004 Mar;18(3):150-7. doi: 10.1097/00005131-200403000-00005. J Orthop Trauma. 2004. PMID: 15091269
-
[Treatment concepts and results in non-infected post-traumatic pseudarthroses of the femur and tibia].Zentralbl Chir. 1994;119(10):706-13. Zentralbl Chir. 1994. PMID: 7801709 German.
-
The treatment of infected nonunion of the tibia following intramedullary nailing by the Ilizarov method.Injury. 2010 Mar;41(3):294-9. doi: 10.1016/j.injury.2009.09.013. Injury. 2010. PMID: 20176169
-
The treatment of infected tibial nonunion by bone transport using the Ilizarov external fixator and a systematic review of infected tibial nonunion treated by Ilizarov methods.Acta Orthop Belg. 2014 Sep;80(3):426-35. Acta Orthop Belg. 2014. PMID: 26280618
-
A systematic review and meta-analysis:comparing the efficacy of the Ilizarov technique alone with lengthening over a nail for lower extremity bone defects.BMC Musculoskelet Disord. 2024 Sep 2;25(1):699. doi: 10.1186/s12891-024-07799-y. BMC Musculoskelet Disord. 2024. PMID: 39223554 Free PMC article.
Cited by
-
Reconstruction of massive tibial defect caused by osteomyelitis using induced membrane followed by trifocal bone transport technique: a retrospective study and our experience.BMC Surg. 2021 Dec 15;21(1):419. doi: 10.1186/s12893-021-01421-x. BMC Surg. 2021. PMID: 34911504 Free PMC article.
-
Trifocal versus Pentafocal bone transport in segmental tibial defects: a matched comparative analysis for posttraumatic osteomyelitis treatment.BMC Musculoskelet Disord. 2024 May 15;25(1):383. doi: 10.1186/s12891-024-07507-w. BMC Musculoskelet Disord. 2024. PMID: 38750523 Free PMC article.
-
Does Integrated Fixation Provide Benefit in the Reconstruction of Posttraumatic Tibial Bone Defects?Clin Orthop Relat Res. 2015 Oct;473(10):3143-53. doi: 10.1007/s11999-015-4326-6. Clin Orthop Relat Res. 2015. PMID: 25940337 Free PMC article.
-
Delivery of Growth Factors to Enhance Bone Repair.Bioengineering (Basel). 2023 Oct 26;10(11):1252. doi: 10.3390/bioengineering10111252. Bioengineering (Basel). 2023. PMID: 38002376 Free PMC article. Review.
-
A Systematic Review and Meta-Analysis of Combined Antibiotic Spacer with Ilizarov Methods in the Treatment of Infected Nonunion of Tibia.Biomed Res Int. 2021 Jan 16;2021:6668617. doi: 10.1155/2021/6668617. eCollection 2021. Biomed Res Int. 2021. PMID: 33532493 Free PMC article.
References
-
- Aronson J. Current concepts review: limb lengthening, skeletal reconstruction bone transport with the Ilizarov method. J Bone Joint Surg Am. 1997;79:1243–1258. - PubMed
-
- Cierny G, 3rd, Zorn KE. Segmental tibial defects comparing conventional and Ilizarov methodology. Clin Orthop Relat Res. 1994;301:118–123. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
