

Hospitalization burden and survival among older glioblastoma patients
- PMID: 24778086
- PMCID: PMC4201065
- DOI: 10.1093/neuonc/nou060
Hospitalization burden and survival among older glioblastoma patients
Abstract
Background: Half of all glioblastoma patients are at least 65 years old. The frequency and duration of hospitalization from disease- and treatment-related morbidity in this population are unknown.
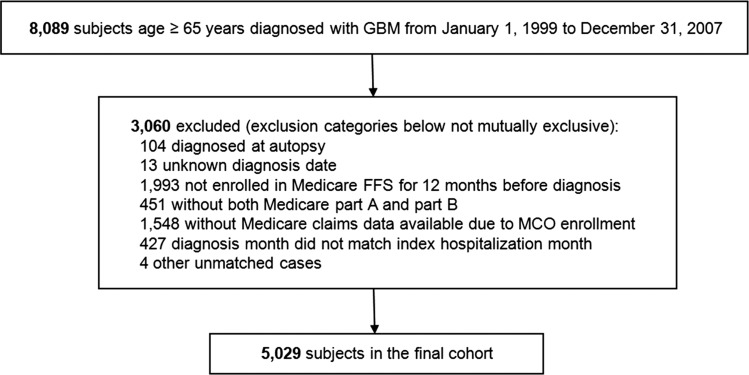
Methods: We performed a retrospective cohort study among patients aged 65 years and older with glioblastoma diagnosed between 1999 and 2007 using SEER-Medicare linked data. Diagnoses and procedures were identified using administrative claims data. Logistic regression was performed to identify predictors of high hospitalization burden.
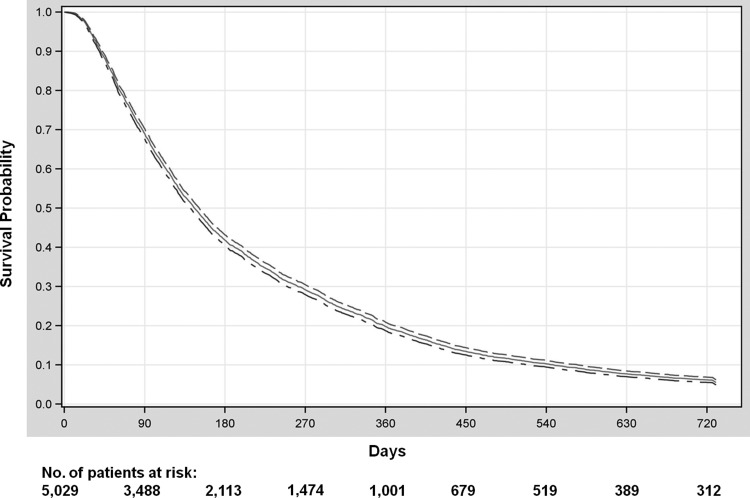
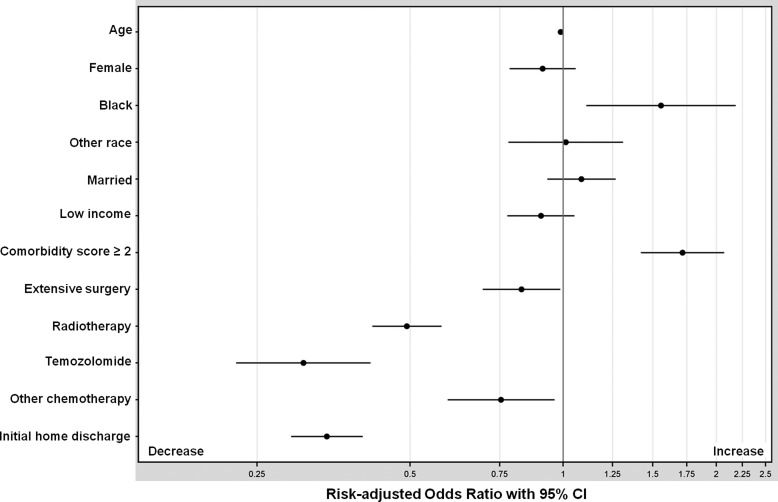
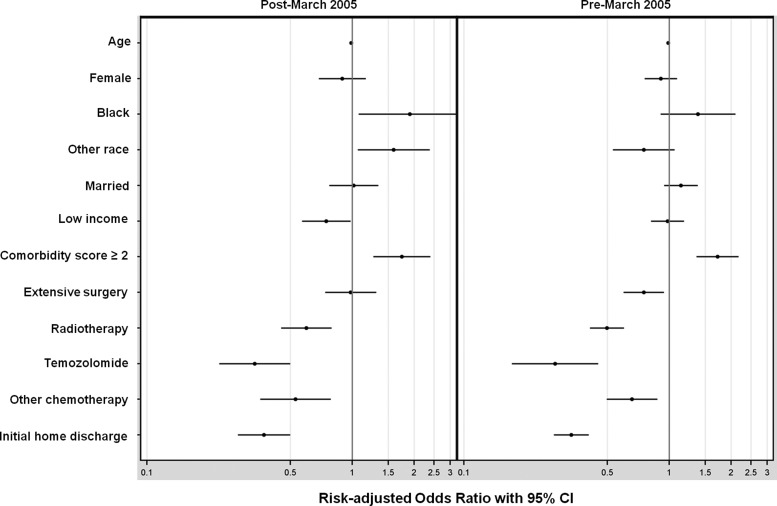
Results: Among the 5029 patients in the cohort, 52% were ages 65-74, and 52% were male. Twenty-six percent of patients underwent extensive resection, 72% received radiotherapy, and 18% received temozolomide. Median survival was 4.9 months. Among all patients, 21% were hospitalized at least 30 cumulative days between diagnosis and death, and 22% of all patients spent at least one-fourth of their remaining lives as inpatients. Higher comorbidity score (adjusted hazard ratio [AHR], 1.72; 95% CI, 1.42-2.07) and black race (AHR, 1.56; 95% CI, 1.11-2.18) were associated with an increased risk of being hospitalized for at least 25% of remaining life, whereas radiation (AHR, 0.49; 95% CI, 0.42-0.58), temozolomide (AHR, 0.31; 95% CI, 0.23-0.42), and extensive surgery (AHR, 0.83; 95% CI, 0.69-0.99) were associated with a decreased risk.
Conclusions: These data highlight the burden of hospitalization faced by a large proportion of older glioblastoma patients. In the setting of short survival, strategies to reduce the amount of time these patients spend hospitalized are urgently needed, to help maintain quality of life at the end of life.
Keywords: elderly; glioblastoma; hospitalization; survival; temozolomide.
© The Author(s) 2014. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Incidence, risk factors, and reasons for hospitalization among glioblastoma patients receiving chemoradiation.J Neurooncol. 2015 Aug;124(1):137-46. doi: 10.1007/s11060-015-1820-3. Epub 2015 Jun 2. J Neurooncol. 2015. PMID: 26033544
-
Patterns of care and outcome for patients with glioblastoma diagnosed during 2008-2010 in Spain.Neuro Oncol. 2013 Jun;15(6):797-805. doi: 10.1093/neuonc/not013. Epub 2013 Mar 3. Neuro Oncol. 2013. PMID: 23460319 Free PMC article.
-
Temozolomide versus standard 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma: the Nordic randomised, phase 3 trial.Lancet Oncol. 2012 Sep;13(9):916-26. doi: 10.1016/S1470-2045(12)70265-6. Epub 2012 Aug 8. Lancet Oncol. 2012. PMID: 22877848 Clinical Trial.
-
Prognosis of patients with multifocal glioblastoma: a case-control study.J Neurosurg. 2012 Oct;117(4):705-11. doi: 10.3171/2012.7.JNS12147. Epub 2012 Aug 24. J Neurosurg. 2012. PMID: 22920963
-
Glioblastoma care in the elderly.Cancer. 2016 Jan 15;122(2):189-97. doi: 10.1002/cncr.29742. Epub 2015 Nov 30. Cancer. 2016. PMID: 26618888 Review.
Cited by
-
Palliative Care in Patients With High-Grade Gliomas in the Neurological Intensive Care Unit.Neurohospitalist. 2020 Jul;10(3):163-167. doi: 10.1177/1941874419869714. Epub 2019 Sep 16. Neurohospitalist. 2020. PMID: 32549938 Free PMC article.
-
Incidence, risk factors, and reasons for hospitalization among glioblastoma patients receiving chemoradiation.J Neurooncol. 2015 Aug;124(1):137-46. doi: 10.1007/s11060-015-1820-3. Epub 2015 Jun 2. J Neurooncol. 2015. PMID: 26033544
-
Glioblastoma in the oldest old: Clinical characteristics, therapy, and outcome in patients aged 80 years and older.Neurooncol Pract. 2023 Oct 20;11(2):132-141. doi: 10.1093/nop/npad070. eCollection 2024 Apr. Neurooncol Pract. 2023. PMID: 38496908 Free PMC article.
-
Palliative Care Service Utilization and Advance Care Planning for Adult Glioblastoma Patients: A Systematic Review.Cancers (Basel). 2021 Jun 8;13(12):2867. doi: 10.3390/cancers13122867. Cancers (Basel). 2021. PMID: 34201260 Free PMC article. Review.
-
Comparative effectiveness of radiotherapy with vs. without temozolomide in older patients with glioblastoma.J Neurooncol. 2017 Jan;131(2):301-311. doi: 10.1007/s11060-016-2294-7. Epub 2016 Oct 21. J Neurooncol. 2017. PMID: 27770280 Free PMC article.
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Iwamoto FM, Reiner AS, Panageas KS, et al. Patterns of care in elderly glioblastoma patients. Ann Neurol. 2008;64(6):628–634. - PubMed
-
- Barnholtz-Sloan JS, Maldonado JL, Williams VL, et al. Racial/ethnic differences in survival among elderly patients with a primary glioblastoma. J Neurooncol. 2007;85(2):171–180. - PubMed
-
- Malmström A, Gronberg BG, Marosi C, et al. Temozolomide versus standard 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma: the Nordic randomised, phase 3 trial. Lancet Oncol. 2012;13(9):916–926. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
