

Bone Plug Versus Suture-Only Fixation of Meniscal Grafts: Effect on Joint Contact Mechanics During Simulated Gait
- PMID: 24778265
- PMCID: PMC4212053
- DOI: 10.1177/0363546514530867
Bone Plug Versus Suture-Only Fixation of Meniscal Grafts: Effect on Joint Contact Mechanics During Simulated Gait
Abstract
Background: Meniscus allograft transplantation (MAT) is primarily undertaken to relieve the symptoms associated with meniscal deficiencies. However, its ability to restore normal knee joint contact mechanics under physiological loads is still unclear.
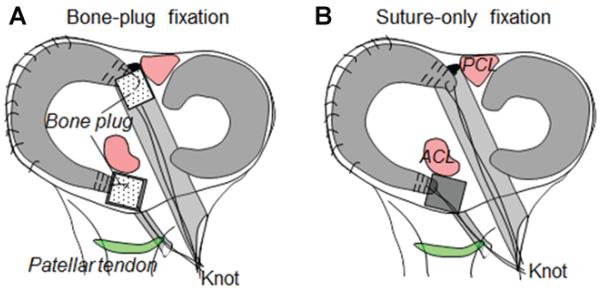
Purpose: To quantify the dynamic contact mechanics associated with 2 commonly used fixation techniques in MAT of the medial compartment: transosseous suture fixation via bone plugs and suture-only fixation at the horns.
Study design: Controlled laboratory study.
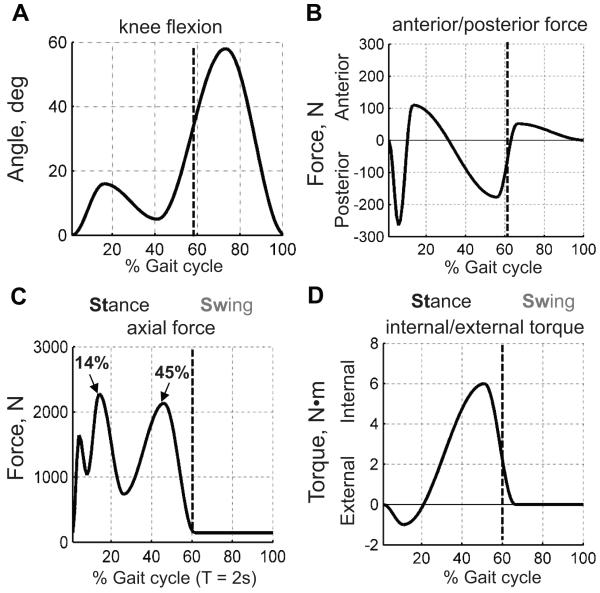
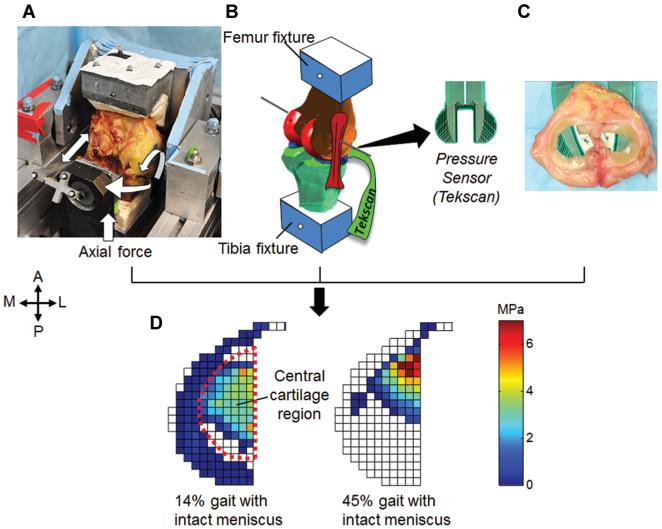
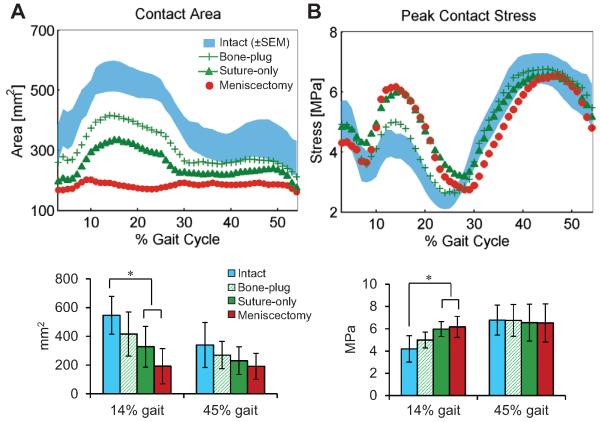
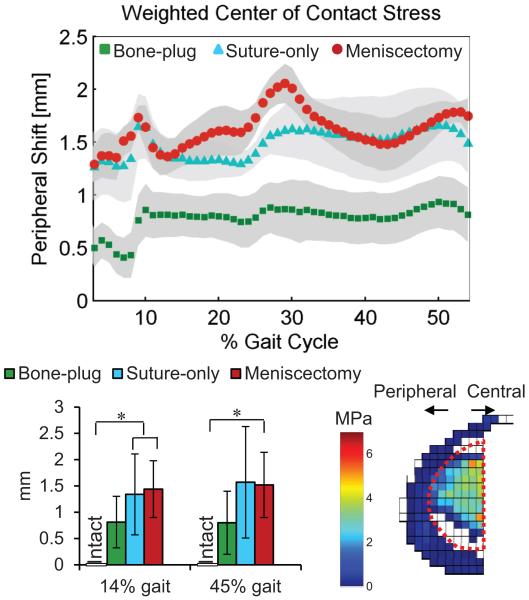
Methods: Physiological loads to mimic gait were applied across 7 human cadaveric knees on a simulator. A sensor placed on the medial tibial plateau recorded dynamic contact stresses under the following conditions: (1) intact meniscus, (2) MAT using transosseous suture fixation via bone plugs at the anterior and posterior horns, (3) MAT using suture-only fixation, and (4) total medial meniscectomy. A "remove-replace" procedure was performed to place the same autograft for both MAT conditions to minimize the variability in graft size, geometry, and material property and to isolate the effects of the fixation technique. Contact stress, contact area, and weighted center of contact stress (WCoCS) were quantified on the medial plateau throughout the stance phase.
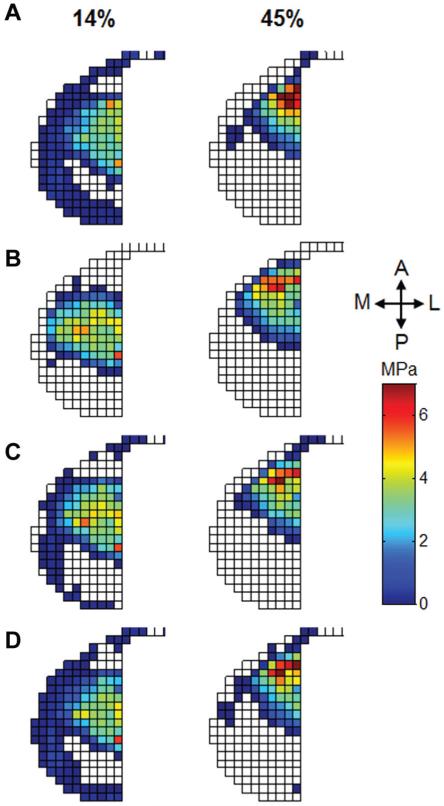
Results: Knee joint contact mechanics were sensitive to the meniscal condition primarily during the first half of the gait cycle. After meniscectomy, the mean peak contact stress increased from 4.2 ± 1.2 MPa to 6.2 ± 1.0 MPa (P = .04), and the mean contact area decreased from 546 ± 132 mm2 to 192 ± 122 mm2 (P = .01) compared with the intact meniscus during early stance (14% of the gait cycle). After MAT, the mean contact stress significantly decreased with bone plug fixation (5.0 ± 0.7 MPa) but not with suture-only fixation (5.9 ± 0.7 MPa). Both fixation techniques partially restored the contact area, but bone plug fixation restored it closer to the intact condition. The location of WCoCS in the central cartilage region (not covered by the meniscus) shifted peripherally throughout the stance phase. Bone plug fixation exhibited correction to this peripheral offset, but suture-only fixation did not.
Conclusion: Under dynamic loading, transosseous fixation at the meniscal horns provides superior load distribution at the involved knee compartment after meniscal transplantation compared with suture-only fixation. Particular attention should be directed to the ability of medial MAT to function during the early stance phase.
Clinical relevance: Transosseous fixation via bone plugs provides superior load distribution of a transplanted meniscal allograft compared with suture fixation alone at time zero.
Keywords: knee; mechanics; meniscus; simulated gait; sports trauma.
© 2014 The Author(s).
Figures
Similar articles
-
Lateral Meniscal Graft Transplantation: Effect of Fixation Method on Joint Contact Mechanics During Simulated Gait.Am J Sports Med. 2019 Aug;47(10):2437-2443. doi: 10.1177/0363546519860113. Epub 2019 Jul 17. Am J Sports Med. 2019. PMID: 31314996 Free PMC article.
-
Lateral Meniscal Allograft Transplantation With Bone Block and Suture-Only Techniques Partially Restores Knee Kinematics and Forces.Am J Sports Med. 2019 Aug;47(10):2427-2436. doi: 10.1177/0363546519858085. Epub 2019 Jun 28. Am J Sports Med. 2019. PMID: 31251657
-
Effect of meniscus replacement fixation technique on restoration of knee contact mechanics and stability.Mol Cell Biomech. 2011 Jun;8(2):123-34. Mol Cell Biomech. 2011. PMID: 21608413
-
Meniscal substitutes--human experience.Scand J Med Sci Sports. 1999 Jun;9(3):146-57. doi: 10.1111/j.1600-0838.1999.tb00445.x. Scand J Med Sci Sports. 1999. PMID: 10380271 Review.
-
Incidence and Extent of Graft Extrusion following Meniscus Allograft Transplantation.Biomed Res Int. 2018 Mar 25;2018:5251910. doi: 10.1155/2018/5251910. eCollection 2018. Biomed Res Int. 2018. PMID: 29770332 Free PMC article. Review.
Cited by
-
Meniscus Allograft Transplantation With Bone Plugs Using Knotless All-Suture Anchors and Cortical Button Suspensory Fixation.Arthrosc Tech. 2023 Sep 11;12(10):e1707-e1714. doi: 10.1016/j.eats.2023.05.020. eCollection 2023 Oct. Arthrosc Tech. 2023. PMID: 37942117 Free PMC article.
-
Tear patterns and locations are different between lateral and medial compartments in patients with early anatomical failure after meniscal allograft transplantation.Knee Surg Sports Traumatol Arthrosc. 2023 Oct;31(10):4485-4491. doi: 10.1007/s00167-023-07506-9. Epub 2023 Aug 18. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 37596367
-
Next Generation Tissue Engineering of Orthopedic Soft Tissue-to-Bone Interfaces.MRS Commun. 2017 Sep;7(3):289-308. doi: 10.1557/mrc.2017.91. Epub 2017 Oct 3. MRS Commun. 2017. PMID: 29333332 Free PMC article.
-
A model system for developing a tissue engineered meniscal enthesis.Acta Biomater. 2017 Jul 1;56:110-117. doi: 10.1016/j.actbio.2016.10.040. Epub 2016 Oct 29. Acta Biomater. 2017. PMID: 27989921 Free PMC article.
-
[Indication and limitations of meniscus replacement].Orthopade. 2017 Oct;46(10):831-838. doi: 10.1007/s00132-017-3469-4. Orthopade. 2017. PMID: 28887704 Review. German.
References
-
- Abat F, Gelber PE, Erquicia JI, Pelfort X, Gonzalez-Lucena G, Monllau JC. Suture-only fixation technique leads to a higher degree of extrusion than bony fixation in meniscal allograft transplantation. Am J Sports Med. 2012;40(7):1591–1596. - PubMed
-
- Abat F, Gelber PE, Erquicia JI, Tey M, Gonzalez-Lucena G, Monllau JC. Prospective comparative study between two different fixation techniques in meniscal allograft transplantation. Knee Surg Sports Traumatol Arthrosc. 2013;21(7):1516–1522. - PubMed
-
- Ahn JH, Bae TS, Kang KS, Kang SY, Lee SH. Longitudinal tear of the medial meniscus posterior horn in the anterior cruciate ligament-deficient knee significantly influences anterior stability. Am J Sports Med. 2011;39(10):2187–2193. - PubMed
-
- Alhalki MM, Howell SM, Hull ML. How three methods for fixing a medial meniscal autograft affect tibial contact mechanics. Am J Sports Med. 1999;27(3):320–328. - PubMed
-
- Alhalki MM, Hull ML, Howell SM. Contact mechanics of the medial tibial plateau after implantation of a medial meniscal allograft: a human cadaveric study. Am J Sports Med. 2000;28(3):370–376. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
