

Use of labour induction and risk of cesarean delivery: a systematic review and meta-analysis
- PMID: 24778358
- PMCID: PMC4049989
- DOI: 10.1503/cmaj.130925
Use of labour induction and risk of cesarean delivery: a systematic review and meta-analysis
Abstract
Background: Induction of labour is common, and cesarean delivery is regarded as its major complication. We conducted a systematic review and meta-analysis to investigate whether the risk of cesarean delivery is higher or lower following labour induction compared with expectant management.
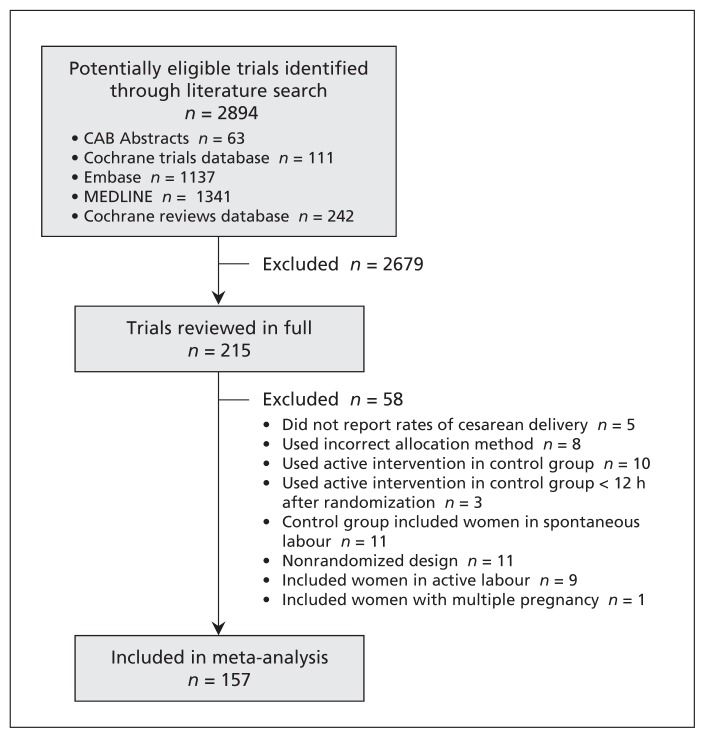
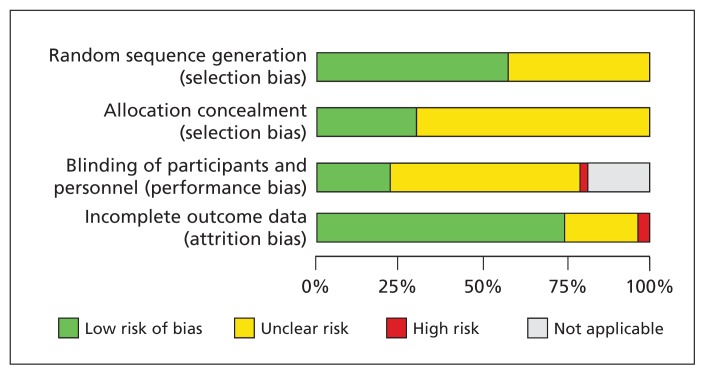
Methods: We searched 6 electronic databases for relevant articles published through April 2012 to identify randomized controlled trials (RCTs) in which labour induction was compared with placebo or expectant management among women with a viable singleton pregnancy. We assessed risk of bias and obtained data on rates of cesarean delivery. We used regression analysis techniques to explore the effect of patient characteristics, induction methods and study quality on risk of cesarean delivery.
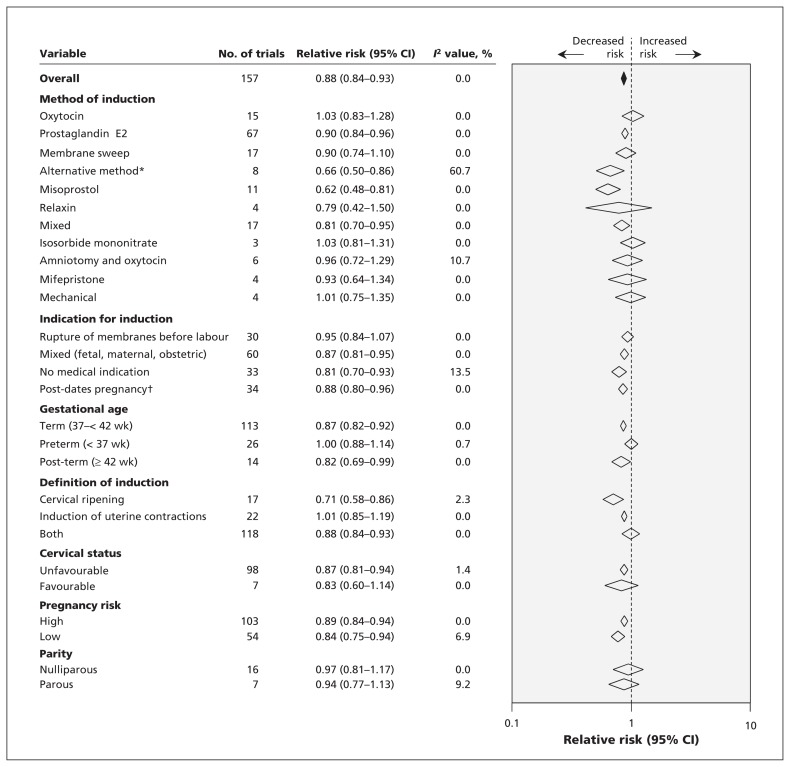
Results: We identified 157 eligible RCTs (n = 31,085). Overall, the risk of cesarean delivery was 12% lower with labour induction than with expectant management (pooled relative risk [RR] 0.88, 95% confidence interval [CI] 0.84-0.93; I(2) = 0%). The effect was significant in term and post-term gestations but not in preterm gestations. Meta-regression analysis showed that initial cervical score, indication for induction and method of induction did not alter the main result. There was a reduced risk of fetal death (RR 0.50, 95% CI 0.25-0.99; I(2) = 0%) and admission to a neonatal intensive care unit (RR 0.86, 95% CI 0.79-0.94), and no impact on maternal death (RR 1.00, 95% CI 0.10-9.57; I(2) = 0%) with labour induction.
Interpretation: The risk of cesarean delivery was lower among women whose labour was induced than among those managed expectantly in term and post-term gestations. There were benefits for the fetus and no increased risk of maternal death.
© 2014 Canadian Medical Association or its licensors.
Figures
Comment in
-
Induction of labour decreases a woman's chance of caesarean delivery when compared with expectant management.Evid Based Med. 2014 Dec;19(6):217. doi: 10.1136/ebmed-2014-110067. Epub 2014 Sep 2. Evid Based Med. 2014. PMID: 25185269 No abstract available.
-
Induction of labour.CMAJ. 2014 Nov 4;186(16):1246. doi: 10.1503/cmaj.114-0077. CMAJ. 2014. PMID: 25367921 Free PMC article. No abstract available.
-
Induction of labour.CMAJ. 2014 Nov 4;186(16):1246-7. doi: 10.1503/cmaj.114-0076. CMAJ. 2014. PMID: 25367922 Free PMC article. No abstract available.
-
The authors respond.CMAJ. 2014 Nov 4;186(16):1247. doi: 10.1503/cmaj.114-0078. CMAJ. 2014. PMID: 25367923 Free PMC article. No abstract available.
-
[Use of labor induction reduces the risk of cesarean section].Perspect Infirm. 2014 Nov-Dec;11(5):53. Perspect Infirm. 2014. PMID: 25438436 French. No abstract available.
References
-
- ACOG Committee on Practice Bulletins — Obstetrics. ACOG Practice Bulletin no 107: induction of labor. Obstet Gynecol 2009; 114:386–97 - PubMed
-
- Induction of labour [clinical guideline 70]. London (UK): National Institute for Health and Clinical Excellence; 2008
-
- Liu DTY, Fairweather DVI. Labour ward manual. Philadelphia (PA): Elsevier; 2007
-
- Induction of labour: evidence-based clinical guideline number 9. London (UK): Royal College of Obstetricians and Gynaecologists Press; 2001
-
- Caughey AB, Sundaram V, Kaimal AJ, et al. Systematic review: elective induction of labor versus expectant management of pregnancy. Ann Intern Med 2009;151:252–63, W53–63 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous