

Liver volumetry: Is imaging reliable? Personal experience and review of the literature
- PMID: 24778768
- PMCID: PMC4000610
- DOI: 10.4329/wjr.v6.i4.62
Liver volumetry: Is imaging reliable? Personal experience and review of the literature
Abstract
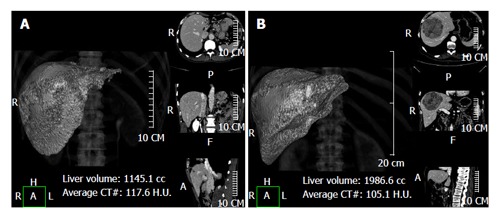
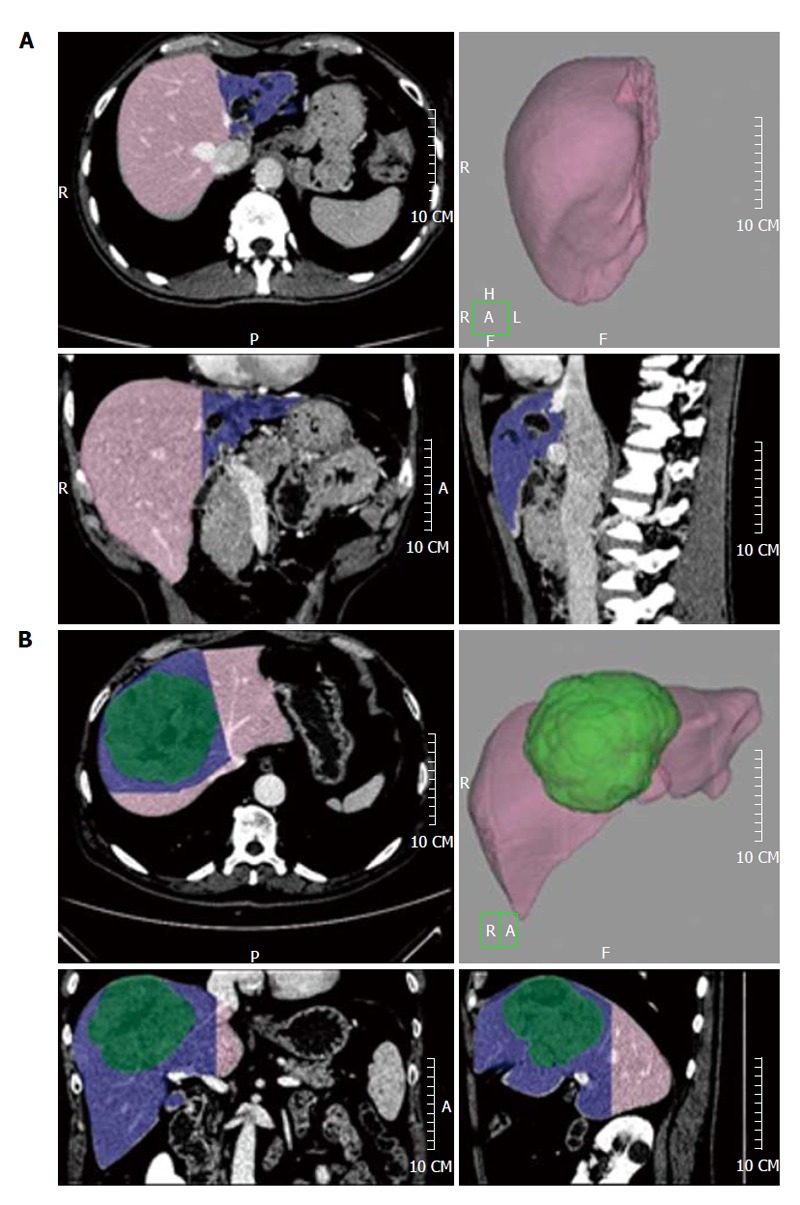
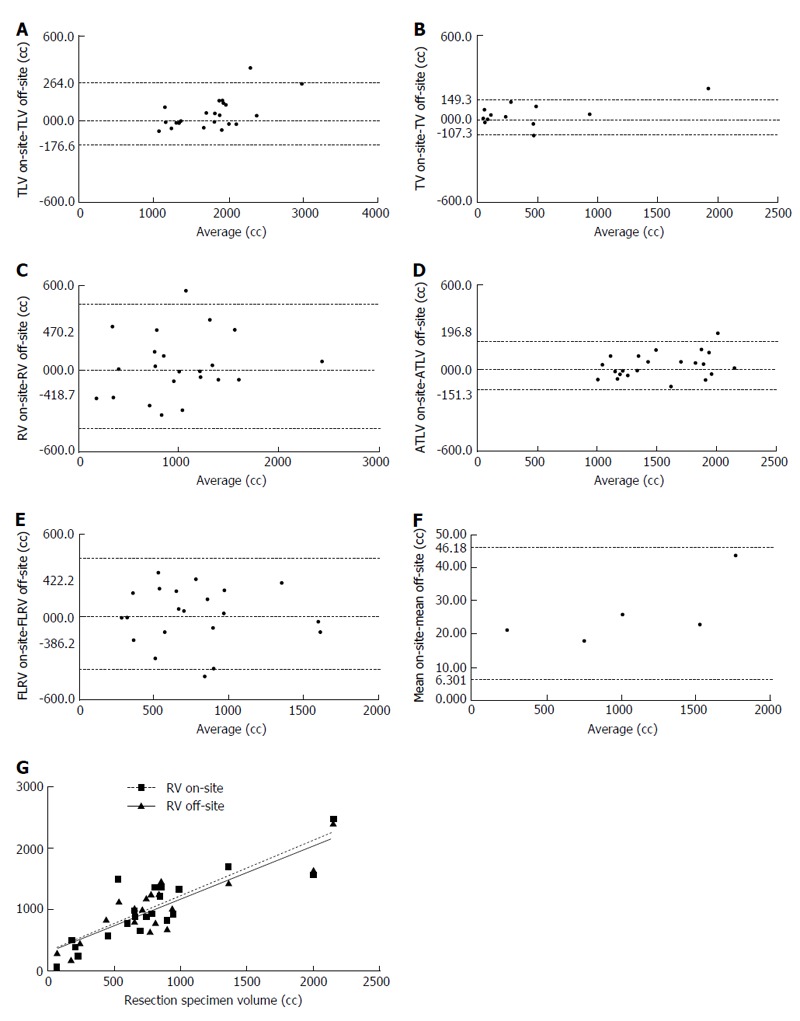
The amount of the future liver remnant volume is fundamental for hepato-biliary surgery, representing an important potential risk-factor for the development of post-hepatectomy liver failure. Despite this, there is no uniform consensus about the amount of hepatic parenchyma that can be safely resected, nor about the modality that should be chosen for this evaluation. The pre-operative evaluation of hepatic volume, along with a precise identification of vascular and biliar anatomy and variants, are therefore necessary to reduce surgical complications, especially for extensive resections. Some studies have tried to validate imaging methods [ultrasound, computed tomography (CT), magnetic resonance imaging] for the assessment of liver volume, but there is no clear evidence about the most accurate method for this evaluation. Furthermore, this volumetric evaluation seems to have a certain degree of error, tending to overestimate the actual hepatic volume, therefore some conversion factors, which should give a more reliable evaluation of liver volume, have been proposed. It is widespread among non-radiologists the use of independent software for an off-site volumetric analysis, performed on digital imaging and communications in medicine images with their own personal computer, but very few studies have provided a validation of these methods. Moreover, while the pre-transplantation volumetric assessment is fundamental, it remains unclear whether it should be routinely performed in all patients undergoing liver resection. In this editorial the role of imaging in the estimation of liver volume is discussed, providing a review of the most recent literature and a brief personal series of correlations between liver volumes and resection specimens' weight, in order to assess the precision of the volumetric CT evaluation.
Keywords: Computed tomography; Hepatectomy; Liver; Magnetic resonance imaging; Ultrasound.
Figures

Similar articles
-
Virtual liver resection and volumetric analysis of the future liver remnant using open source image processing software.World J Surg. 2010 Oct;34(10):2426-33. doi: 10.1007/s00268-010-0663-5. World J Surg. 2010. PMID: 20652701 Free PMC article.
-
Novel three-dimensional imaging technique improves the accuracy of hepatic volumetric assessment.HPB (Oxford). 2011 Sep;13(9):670-4. doi: 10.1111/j.1477-2574.2011.00350.x. Epub 2011 Jul 19. HPB (Oxford). 2011. PMID: 21843269 Free PMC article.
-
Prospective volumetric assessment of the liver on a personal computer by nonradiologists prior to partial hepatectomy.World J Surg. 2011 Feb;35(2):386-92. doi: 10.1007/s00268-010-0877-6. World J Surg. 2011. PMID: 21136056 Free PMC article.
-
Hepatic function assessment to predict post-hepatectomy liver failure: what can we trust? A systematic review.Updates Surg. 2020 Dec;72(4):925-938. doi: 10.1007/s13304-020-00859-7. Epub 2020 Aug 4. Updates Surg. 2020. PMID: 32749596
-
CT and MR imaging evaluation of living liver donors.Abdom Radiol (NY). 2021 Jan;46(1):17-28. doi: 10.1007/s00261-019-02385-6. Abdom Radiol (NY). 2021. PMID: 31901101 Review.
Cited by
-
Post-hepatectomy liver failure.Hepatobiliary Surg Nutr. 2014 Oct;3(5):238-46. doi: 10.3978/j.issn.2304-3881.2014.09.01. Hepatobiliary Surg Nutr. 2014. PMID: 25392835 Free PMC article. Review.
-
FIRST BRAZILIAN CONSENSUS ON MULTIMODAL TREATMENT OF COLORECTAL LIVER METASTASES. MODULE 1: PRE-TREATMENT EVALUATION.Arq Bras Cir Dig. 2015 Nov-Dec;28(4):222-30. doi: 10.1590/S0102-6720201500040002. Arq Bras Cir Dig. 2015. PMID: 26734788 Free PMC article.
-
Magnetic Resonance Imaging Liver Segmentation Protocol Enables More Consistent and Robust Annotations, Paving the Way for Advanced Computer-Assisted Analysis.Diagnostics (Basel). 2024 Dec 11;14(24):2785. doi: 10.3390/diagnostics14242785. Diagnostics (Basel). 2024. PMID: 39767146 Free PMC article.
-
The correlation between preoperative volumetry and real graft weight: comparison of two volumetry programs.Ann Surg Treat Res. 2017 Apr;92(4):214-220. doi: 10.4174/astr.2017.92.4.214. Epub 2017 Mar 24. Ann Surg Treat Res. 2017. PMID: 28382294 Free PMC article.
-
The value of intraoperative dynamic liver function test ICG in predicting postoperative complications in patients undergoing staged hepatectomy: a pilot study.Langenbecks Arch Surg. 2023 Jul 5;408(1):264. doi: 10.1007/s00423-023-02983-5. Langenbecks Arch Surg. 2023. PMID: 37403000 Free PMC article.
References
-
- Scheele J, Stangl R, Altendorf-Hofmann A. Hepatic metastases from colorectal carcinoma: impact of surgical resection on the natural history. Br J Surg. 1990;77:1241–1246. - PubMed
-
- Scheele J. [Vasculature based segmental resection of the liver] Langenbecks Arch Chir. 1990;375:308–317. - PubMed
-
- Okamoto E, Kyo A, Yamanaka N, Tanaka N, Kuwata K. Prediction of the safe limits of hepatectomy by combined volumetric and functional measurements in patients with impaired hepatic function. Surgery. 1984;95:586–592. - PubMed
-
- Cohnert TU, Rau HG, Buttler E, Hernandez-Richter T, Sauter G, Reuter C, Schildberg FW. Preoperative risk assessment of hepatic resection for malignant disease. World J Surg. 1997;21:396–400; discussion 401. - PubMed
-
- Rau HG, Schauer R, Helmberger T, Holzknecht N, von Rückmann B, Meyer L, Buttler E, Kessler M, Zahlmann G, Schuhmann D, et al. Impact of virtual reality imaging on hepatic liver tumor resection: calculation of risk. Langenbecks Arch Surg. 2000;385:162–170. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
