

Latissimus dorsi free flap reconstruction of major abdominal defect in treatment of giant Marjolin's ulcer: a short report focused on preoperative imaging
- PMID: 24778800
- PMCID: PMC4001431
- DOI: 10.1177/2047981613516614
Latissimus dorsi free flap reconstruction of major abdominal defect in treatment of giant Marjolin's ulcer: a short report focused on preoperative imaging
Abstract
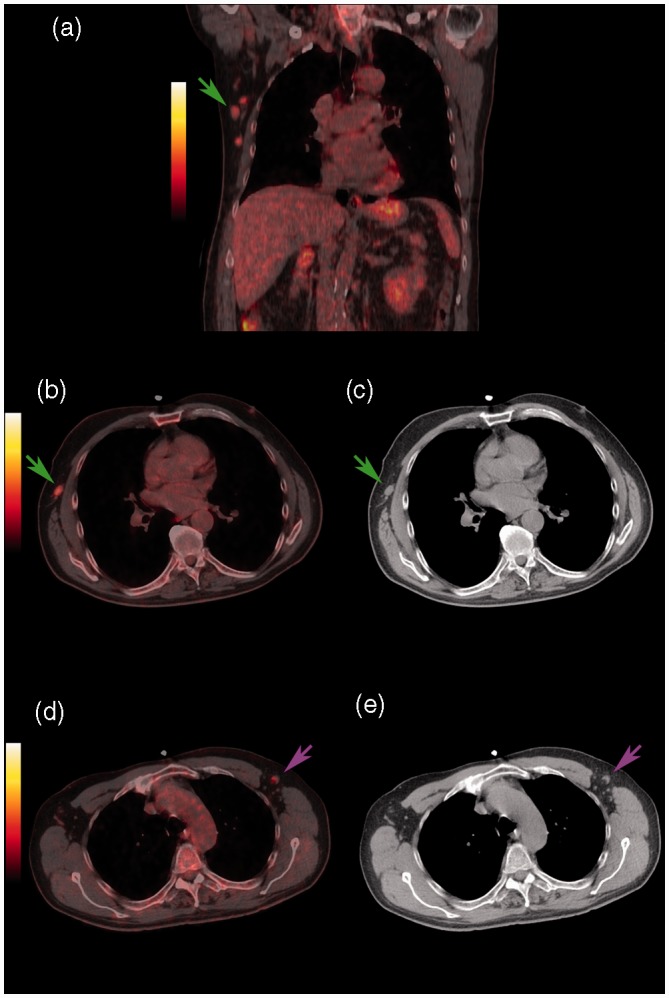
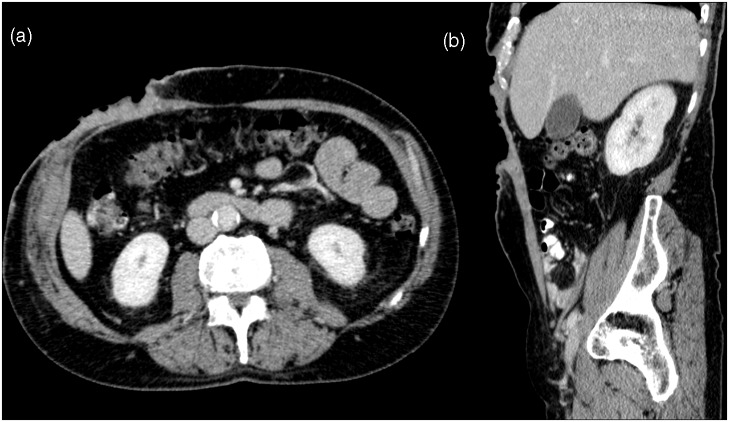
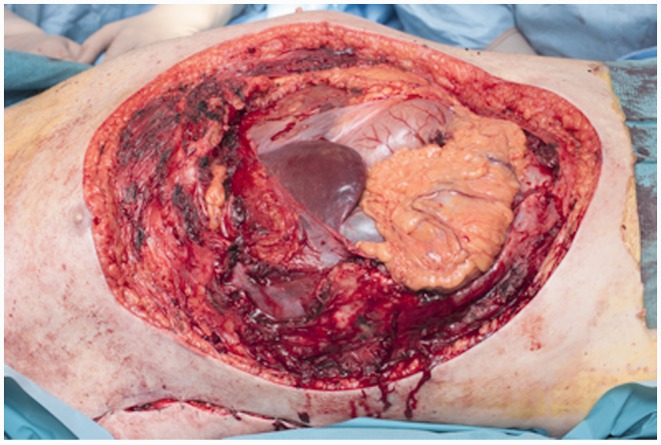
We present a case of a 56-year-old man with a giant carcinoma in the abdominal wall. Based on positron emission tomography/computed tomography (PET/CT) scan there were FDG-avid lymph nodes in the ipsilateral axillary and groin, suspicious for metastases. At contrast-enhanced CT the parietal peritoneum seemed free of tumor invasion, which was essential to radical surgery planning. The tumor was completely removed with clear margins of resection and no metastasis in the resected lymph nodes. The PET/CT scan was repeated after 4 months, showing no signs of recurrence.
Keywords: Positron emission tomography (PET); computed tomography (CT); metastases; soft tissues/skin; surgery.
Figures


References
-
- Fleming MD, Hunt JL, Purdue GF, et al. Marjolin’s ulcer: a review and reevaluation of a difficult problem. J Burn Care Rehabil 1990; 11: 460–469. - PubMed
-
- Copcu E, Aktas A, Sişman N, et al. Thirty-one cases of Marjolin’s ulcer. Clin Exp Dermatol 2003; 28: 138–141. - PubMed
-
- Novick M, Gard DA, Hardy SB, et al. Burn scar carcinoma: a review and analysis of 46 cases. J Trauma 1977; 17: 809–817. - PubMed
-
- Jensen JPN, Alsbjørn BF. Cancerudvikling i cikatricielt væv og sår [in Danish: Formation of cancer in scars and ulcers]. Sår 1994; 2: 18–22.
-
- Esther RJ, Lamps L, Schwartz HS. Marjolin ulcers: secondary carcinomas in chronic wounds. J South Orthop Assoc 1999; 8: 181–187. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources